Life Extension Magazine®

CDC Says: 200,000 Americans Die Needlessly Every Year
In 2013, the Centers for Disease Control reported that nearly 200,000 avoidable deaths occur each year in the United States from vascular diseases. The CDC described simple changes that can slash risk factors before heart attack or stroke strikes. Life Extension® points out that even more lives could be spared with vigilant annual blood testing.
Scientifically reviewed by Dr. Gary Gonzalez, MD, in October 2024. Written by: William Faloon.

The Centers for Disease Control and Prevention (CDC) deserve a level of respect that does not exist with most bureaucracies.
When the first cases of AIDS were reported in the United States in 1981, the CDC knew this country faced a contagious disease crisis and took action.
Despite interference by other government agencies, the CDC persisted with meticulous research. Within 18 months the CDC identified all the major risk factors for acquired immune deficiency syndrome (AIDS).1
The Food and Drug Administration (FDA), on the other hand, responded by organizing armed raids against those who sought novel ways to prevent the immune deficits that were ravaging AIDS patients.2
Life Extension ® was one victim of these police-state actions. We were fortunate that our early recommendations were vindicated before the FDA could incarcerate us.3-5
In 2013, the CDC released a report estimating that nearly 200,000 avoidable deaths occur each year in the United States from heart disease, stroke, and hypertensive disorders.6
According to the CDC, prevention of vascular disease can be as simple as following the “ABCS”, which stands for: “aspirin, blood pressure control, cholesterol management, and smoking cessation.”7
Life Extension does not question the accuracy of this CDC report. We in fact believe it to be understated. Our concern is that the CDC report contains omissions about other preventable causes of vascular disease overlooked by hurried physicians.

This article will show why the number of needless deaths is higher than the CDC estimates and how you can avoid being a victim.
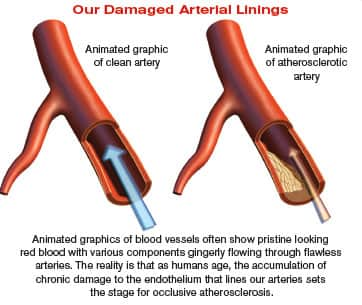
Atherosclerosis is the term used to describe damage and obstruction to the linings of our arteries.8 When arterial blood flow is impeded or blocked, the result can be death or disability from a stroke or heart attack.8
A misconception about atherosclerosis is that it is a modern day scourge caused by unhealthy habits. I’ve heard so-called experts’ claim that people didn’t suffer coronary artery disease in the past because their diets were so natural.
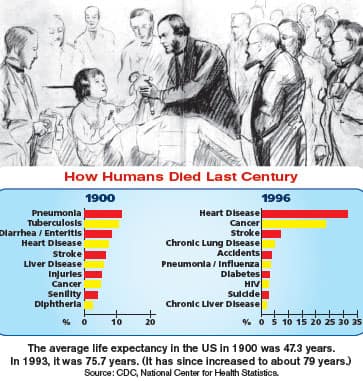
These “experts” had no basis to claim that atherosclerosis is a modern day phenomenon. All they could cite was that few people developed heart disease in the past compared to today. The reason more people weren’t having heart attacks back then was that most died before age 50 from diseases that are now preventable/curable.
A study on this topic published in The Lancet last year attracted worldwide media attention. It documented that mummified human bodies dating back 4,000 years and spanning multiple geographic locations/cultures suffered from clogged arteries.9
As Life Extension has long argued, atherosclerosis is a disease of aging that has always been prevalent. It took MRI imaging to document clear signs of heart disease in 34% of mummified humans whose estimated mean age at death was 43 years. Those who died at an estimated mean age of 32 years were less likely to show signs of atherosclerosis.9
According to the lead investigator of The Lancet study:
“The fact that we found similar levels of atherosclerosis in all of the different cultures we studied, all of whom had very different lifestyles and diets, suggests that atherosclerosis may have been far more common in the ancient world than previously thought,”10
—Randall Thompson, MD
These findings help confirm that atherosclerosis has always been widespread. The encouraging news is that methods to prevent and even reverse it have been validated in modern clinical studies.
What Caused Atherosclerosis In The Mummified Bodies?
In seeking to identify what caused atherosclerosis in the mummified bodies, The Lancet researchers speculated that it could have been the high levels of inflammation these primitive people were exposed to from constant infections and a non-hygienic environment.10
People with severe inflammatory conditions (like rheumatoid arthritis and lupus) suffer accelerated atherosclerosis.11-13 Multiple studies on normal modern people link chronic inflammation as an independent risk factor for stroke and heart attack.14-16
A study published in late 2013 corroborate this. The investigators reported on a large group of older individuals who were followed for 17 years. Those with the highest levels of inflammatory blood markers were over 3 times as likely to suffer sudden cardiac death as those with the lowest levels.17
The recent CDC report did not factor in chronic inflammation as an “avoidable” cause of vascular-related death.1 That’s just one reason why the CDC’s number of avoidable deaths is an underestimate of how many lives could be spared.
It’s comforting to live in an era where chronic inflammation can be identified with blood tests and corrective actions taken to suppress elevated inflammatory markers.
Why Is Atherosclerosis So Common?
We know that excess dietary intake of the wrong kinds of fats and sugars damages our arterial lining, as does tobacco smoke.18-23 Overlooked is the continuous toxic exposure arteries bear to cellular waste products that are released into our bloodstream for filtration and excretion primarily through the kidneys.24
Most of us are born with a flawlessly intact endothelium that lines our arteries and protects against formation of atherosclerosis. As we age, our arterial lining endures chronic insult from internal and external factors that results in loss of blood flow to the heart, kidneys, and brain. This is the leading reason why most aging people today become disabled and then prematurely die.
Those who understand the many causes of atherosclerosis should not be surprised it is so common. What’s appalling is the number of people who continue to succumb to atherosclerotic diseases because of widespread physician apathy and ignorance.
Endothelial Dysfunction: The Villain Behind Atherosclerosis

Multiple culprits initiate and promote atherosclerosis. They share in common an ability to damage the delicate endothelium that lines our vascular systems.25
An early step in the initiation of atherosclerosis is often reduced nitric oxide bioavailability that initiates endothelial dysfunction.26 Aging results in further impairment in the ability to synthesize endothelial nitric oxide that markedly accelerates atherosclerosis.27,28
We are grateful to the many scientists who have conducted research showing that consumption of plant polyphenol concentrates (such as those found in pomegranate,29-31 green tea,32-34 and red grapes)35-39 protect nitric oxide production, thus helping to restore youthful function and structure to our endothelial arterial linings.
It is somewhat contradictory, however, for one to gobble down capsule concentrates of pomegranate, green tea, berries, and grapes and then ignore other proven factors that silently destroy endothelial function.
Elevated glucose,40-42 insulin,43-45 triglycerides,46,47 LDL,48-50 homocysteine,51-53 C-reactive protein,54-56 oxidative stress,57-59 along with low HDL60-62 and low testosterone63,64 (in men) inflict their own unique forms of endothelial damage. It is thus critical to have one’s blood tested annually to ensure that none of these destroyers of endothelial integrity get out of safe ranges.
Vascular Toxicity Of Homocysteine
Elevated homocysteine has been linked to atherosclerosis via several toxic mechanisms.65-69 A few years ago, some studies questioned whether modestly-elevated homocysteine was really a health concern. Life Extension has published extensive information on the dangers of homocysteine as well as rebuttals to studies that the media portrayed in a highly misleading way.70-74
There is now a controversy in the mainstream as to what blood level of homocysteine really poses a vascular disease risk. Children who have a genetic defect that causes extremely high homocysteine levels show signs of impaired endothelial function as early as age 4.75
The question is what blood level of homocysteine should typical aging people strive for. The mainstream defines elevated homocysteine (called hyperhomocysteinemia) as greater than 15 micromoles per liter of blood.76 Other studies suggest that keeping homocysteine far below 15 is advisable.76
High homocysteine is associated with increasing age, consumption of animal protein, smoking, postmenopausal state, sedentary lifestyle, decreased kidney function, deficiencies of B-vitamins or with certain genetic abnormalities.77-83
Failure to test homocysteine blood levels can leave one vulnerable to silent vascular damage and increased dementia risks.76
When one understands the mechanisms by which homocysteine inflicts cellular damage, the importance of keeping it in lower ranges becomes abundantly clear.
How To Slow And Reverse Atherosclerosis
 |
Scientists long ago documented the ability of HDL (high-density lipoprotein) to remove cholesterol affixed to arterial walls and transport it to the liver for safe disposal.
This is why it is so important to maintain HDL levels above 50 mg/dL of blood and follow steps Life Extension has outlined to ensure optimal reverse cholesterol transport of lipids away from the arterial wall.124
HDL does more than just cleanse arterial walls of plaque. It also protects LDL against oxidation, while inhibiting chronic inflammation, vascular adhesion molecules, and platelet activation—all factors that can lead to atherosclerosis. 125-130
For HDL to perform its vital functions, an enzyme called paraoxonase-1 (PON-1) is attached to its surface.130,131
Aging and poor diet result in a marked decline in PON-1 levels, thereby reducing the ability of HDL to protect against heart attack and stroke.132,133 This phenomenon helps explain the onset of accelerated atherosclerosis; where within a period of only a few years, an aging person’s healthy arteries rapidly occlude with plaque.
The age-related reduction in PON-1 may also explain studies showing that statin drugs lose their benefit in certain aging populations, since the effects of statins are no longer sufficient to protect against the multiple factors involved in the development of atherosclerosis in the elderly.134,135
PON-1 is anchored to the surface of HDL and is emerging as a formidable defense against atherosclerosis.130,136,137
Pharmaceutical companies would pay a king’s ransom for a drug that elevates PON-1 levels in the body. Fortunately, scientists have discovered low-cost natural methods (such as pomegranate and resveratrol) to elevate PON-1 and unleash its full antioxidant and anti-inflammatory power.138-142
In studying the effects of pomegranate alone over a one-year period, studies using human serum revealed an 83% increase in PON-1 activity and a 90% decrease in oxidized LDL. These same patients showed reversal in clinical measurements of atherosclerosis such as carotid artery narrowing.143
Homocysteine Damages The Brain
Solid evidence connects the reduced cerebral blood flow with higher Alzheimer’s risk as well as its rapid progression.84-86
A study published in 2013 showed that people with homocysteine levels of 25.5 micromoles/L and higher were almost 4 times as likely to have severe shrinkage of the brain’s temporal lobe and had almost 5 times the risk for a severe brain white matter abnormality.87 This brain damage places people at increased risk of stroke, dementia, and death.88 This study is corroborated by previous studies showing brain benefits when B-vitamins are used to suppress homocysteine.89
The devastating impact that elevated homocysteine has on the brain alone should motivate maturing individuals to check their homocysteine blood level and take appropriate actions to suppress it if elevated.
Fortunately, most people can reduce elevated homocysteine levels by ensuring proper intake of folic acid, vitamin B12, and vitamin B6.90-92
A fatal assumption we have observed in people taking multivitamins is they assume their homocysteine levels are being adequately suppressed. Only a blood test can verify that homocysteine levels are in the safe ranges.
Some individuals, for instance, don’t absorb vitamin B12 well and require a sublingual or injectable route of administration. Others need to take extra vitamin B6 or the more metabolically active L-methylfolate form of folic acid to effectively suppress elevated homocysteine.
Low Testosterone Associated With Higher Vascular Risk
Testosterone levels are high in young men, but plummet during aging.
Low testosterone in men is associated with excess abdominal fat,93,94 loss of insulin sensitivity,95,96 atherosclerosis,97,98 and increased incidence of cardiovascular disease.99
A review of data gathered between 1970 and 2013 provided further evidence that low testosterone in men may be linked to a higher risk of developing or dying from cardiovascular disease.100
Another 2013 study confirmed the increase of metabolic syndrome in men that are testosterone deficient.101 Metabolic syndrome is a cluster of cardiovascular risk factors that include insulin resistance, hypertension, elevated triglycerides/LDL and low HDL.102 This study found that men treated with testosterone showed across the board improvements as indicated by:101
- Reduced LDL.
- Reduced triglycerides.
- Reduced glucose.
- Reduced C-reactive protein.
- Reduced measures of liver damage.
- Reduced blood pressure.
- Reduced hemoglobin A1c.
- Increased HDL (removes cholesterol buildup from arterial walls).
This stream of favorable data is causing testosterone prescriptions to surge. From 1994 to 2004, prescription sales of testosterone increased by 500%.103 We believe they have grown substantially more than that since then, especially when considering that sales of low-cost compounded testosterone creams are not easily counted in the official statistics.
It is regrettable that despite compelling findings of profound efficacy, some conventional doctors still question the value of testosterone replacement in maturing men. This oversight is causing too many needless heart attacks.
For nearly 20 years, Life Extension has urged its male members to restore testosterone levels to youthful ranges. We have written meticulous rebuttal to media attacks that question the value of properly-prescribed natural testosterone.
George W. Bush’s Blocked Coronary Artery
George W. Bush
George W. Bush (the younger Bush) may have been the first President to describe his daily health routine that included regular exercise along with a multivitamin, low-dose aspirin, and possibly some fish oil. Former President Bush had annual physical exams by the government’s best doctors.
In August 2013, doctors discovered that a vital coronary artery in George W. Bush was 95% blocked. An emergency stent was inserted to restore blood flow through the occluded artery. According to medical sources, the location and severity of the coronary artery blockage usually causes sudden death and the former President was lucky his doctors caught it in time.105
We are seeking the medical records of President Bush through the Freedom of Information Act, but we are confident that his annual “Presidential” exams did not include the comprehensive blood testing that Life Extension members take each year. As we long ago documented, all it takes is for one independent vascular risk factor to be out of safe range for a heart attack, stroke or kidney failure to ensue.106-108
Vascular disease was the cause of death of former Presidents Franklin Roosevelt, Harry Truman, Dwight Eisenhower, Lyndon Johnson, Richard Nixon and Gerald Ford. Eisenhower suffered horrifically from heart disease for over a decade before dying from congestive heart failure.109,110
In 2004, Bill Clinton underwent open heart surgery to bypass multiple blocked arteries in his heart that would have likely killed him in a few months if not treated.111 He had to undergo follow-up surgery in 2005 to correct a complication caused by his first bypass surgery.112
In 2010, Clinton was rushed to the hospital complaining of chest pains and had two stents implanted to open two new occluded coronary arteries. Clinton regularly exercised, but did little else other than what his conventional doctors prescribed. Clinton’s program obviously failed to protect him from severe and recurring coronary atherosclerosis.113
Dick Cheney’s Multiple Heart Attacks

Dick Cheney
In this month’s issue, we feature a review of a book authored by former Vice President Dick Cheney.116 Perhaps no living political figure better exemplifies what happens to one’s arteries in response to poor lifestyle choices than Dick Cheney.
Cheney was known for eating outrageous quantities of artery-clogging foods and smoking heavily for 20 years.
Dick Cheney suffered his first heart attack in 1978, when he was only 37. He suffered his second in 1984 and a third in 1988 before undergoing a quadruple bypass surgery to unblock his clogged arteries. His fourth heart attack occurred in 2000. At that time, doctors inserted a stent to open a re-occluded coronary artery.
In 2001, doctors implanted a device to track and control Cheney’s heart rhythm. In 2008, he underwent a procedure to restore his heart to a normal rhythm after doctors found that he was experiencing a recurrence of atrial fibrillation. Despite all this, Cheney suffered his fifth heart attack in February 2010.
Dick Cheney has reportedly taken statin drugs for nearly two decades. In June 2001, his LDL was an excellent 72 mg/dL, indicating he was taking a high-dose statin drug. This did not, however, prevent him from suffering another heart attack.
The former Vice President has had access to the best that conventional cardiology can offer, yet his chronic heart ailments did not abate until he received a heart transplant in 2012.
Don’t Be Victimized By Overwhelmed Doctors
We at Life Extension have new members send us their blood test results for our review. It never ceases to amaze us as to how many important blood tests such as C-reactive protein, hemoglobin A1c, homocysteine, and vital hormones are omitted.
Standard blood panels today look at lipids (cholesterol, LDL, HDL, triglycerides) and glucose. If levels of these vascular risk markers are within conventional “reference ranges,” then the patient is told they are fine.
One big mistake that people make is thinking that being in the “reference range” means they are safe. For instance, a doctor may look at your fasting glucose reading of 97 mg/dL and say you have no diabetic problems. If you happen to be over-secreting large amounts of insulin that keeps your glucose suppressed, then you are facing diabetic complications that can adversely impact every part of your body. A hemoglobin A1c test is a far more accurate measure of glucose control. Fasting glucose levels should be below 86 mg/dL and hemoglobin A1c below 5.6%.)122,123
With restrictions being placed on healthcare expenditures, aging Americans are being denied the opportunity to protect their circulatory system against atherosclerosis. Doctors facing a surge of newly insured patients under the Affordable Care Act are less able to spend the time to evaluate comprehensive blood test results. It is up to the individual to take charge of their health and longevity by having annual blood tests and following up on any reading that is out of optimal range.
Life Extension’s Common Sense Approach
A meticulous review of the scientific literature reveals a multitude of factors that cause humans to accumulate atherosclerotic plaque. Validated blood markers are available to identify specific vascular risks so that corrective actions can be taken before a heart attack or stroke strikes.
Yet this scientific approach to disease prevention is tragically overlooked by today’s hurried medical establishment.
Life Extension retails a comprehensive Male and Female Blood Test Panel for $400. This is a fraction of the price most commercial labs charge for all of these tests you can see outlined on the next page.
Once a year, we sharply discount the member price of the Male or Female Panels to $199. This enables Foundation members to gain control over their medical destiny and initiate meaningful changes before acute or chronic disease ensues.
With increasing insurance deductibles and co-pays, obtaining a comprehensive Male or Female Panel represents a huge economic value. Discovering correctable disease factors not only spares suffering and premature death, but could save tens of thousands of dollars in medical outlays that may not be covered by health insurance.
Elevated Glucose Kills After People Are Hospitalized
 |
Higher hospital admission glucose levels have been shown in several studies to predict increased risk in heart attack patients.117-119 Data also suggest that elevated hemoglobin A1c is associated with an increased risk of cardiovascular disease, even in patients without diabetes.120
For example, a study published in 2013 showed that combined admission glucose and hemoglobin A1c values were independently associated with adverse clinical outcomes in non-diabetic patients with acute coronary syndrome treated with coronary stents or other interventions.121
The take-home message is that glucose need not reach diabetic levels (above 125 mg/dL) to inflict deadly consequences. Optimal fasting glucose levels are below 86 mg/dL.
How Easy It Is To Get Tested…
You can order the Male Panel or Female Panel at these discounted prices by making one phone call to 1-800-208-3444 (24 hours).
Within a few days you’ll receive a listing of blood drawing stations in your neighborhood. Appointments are usually not necessary, meaning you can have your blood drawn at your convenience.
With today’s modern technology, your results come back fast. If you have any questions, you can phone or email our health advisors 7-days a week.
I am often asked what are the most important nutrients, hormones or age-delaying drugs to take. My steadfast answer is that I have no idea what is most important for YOU until I see results from a comprehensive blood test panel.
It does little good to protect your body from say oxidized LDL if your homocysteine and C-reactive protein levels are elevated…or you’re unwittingly taking a drug that is slowly destroying your kidneys or liver.
The Male and Female Blood Test Panels provide a wide range of blood markers to reduce the risk that an insidious minor disorder will someday inflict permanent damage in you.
To order these comprehensive blood test panels at the year’s lowest prices, call 1-800-208-3444 today.
For longer life,
William Faloon
Male and Female Blood Test Panels
Unlike commercial blood tests that evaluate only a few disease risk factors, Life Extension’s Male and Female Blood Test. Panels measure a wide range of blood markers that predispose people to common age-related disorders. Just look at the huge number of parameters included in the Male and Female Blood Test Panels:
| MALE PANEL | FEMALE PANEL |
Lipid ProfileTotal Cholesterol Cardiac MarkersC-Reactive Protein (high sensitivity) HormonesFree and Total Testosterone Metabolic ProfileGlucose Complete Blood Count (CBC)Red Blood Cell count including: hemoglobin, hematocrit, MCV, MCH, MCHC, RDW Cancer MarkerPSA (Prostate Specific Antigen) |
Lipid ProfileTotal Cholesterol Cardiac MarkersC-Reactive Protein (high sensitivity) HormonesProgesterone Metabolic ProfileGlucose Complete Blood Count (CBC)Red Blood Cell count including: hemoglobin, hematocrit, MCV, MCH, MCHC, RDW |
Non-member retail price: $400 • Special Member Discount Price: $199.
Blood Test Super Sale — March 31st through June 2, 2014.
To obtain these comprehensive Male or Female Panels at these low prices,
call 1-800-208-3444 to order your requisition forms.
Then—at your convenience—you can visit one of the blood-drawing facilities provided by LabCorp in your area.
(Restrictions apply in NY, NJ, RI, MA, MD, PA)
References
- Available at: http://www.cdc.gov/mmwr/pdf/wk/mm5021.pdf. Accessed February 13, 2014.
- Available at: http://www.poz.com/articles/263_16238.shtml. Accessed February 13, 2014.
- Available at: https://www.lifeextension.com/offshoredrugs.htm. Accessed February 13, 2014.
- Pedersen C, Sandström E, Petersen CS, et al. The efficacy of inosine pranobex in preventing the acquired immunodeficiency syndrome in patients with human immunodeficiency virus infection. The Scandinavian Isoprinosine Study Group. N Engl J Med. 1990 Jun 21;322(25):1757-63.
- Available at: http://www.cryonet.org/cgi-bin/dsp.cgi?msg=446. Accessed February 13, 2014.
- Available at: http://thechart.blogs.cnn.com/2013/09/03/cdc-200000-people-die-needlessly-every-year. Accessed January 29, 2014.
- Available at: http://www.cdc.gov/dhdsp/vital_signs.htm. Accessed January 29, 2014.
- Available at: https://www.nhlbi.nih.gov/health/health-topics/topics/atherosclerosis. Accessed February 13, 2014.
- Thompson RC, Allam AH, Lombardi GP, et al. Atherosclerosis across 4000 years of human history: the Horus study of four ancient populations. Lancet . 2013 Apr 6;381(9873):1211-22.
- Available at: http://vitals.nbcnews.com/_news/2013/03/10/17260261-mummy-study-shows-clogged-arteries-are-nothing-new?lite. Accessed February 14, 2014.
- Tanasescu C, Jurcut C, Jurcut R, Ginghina C. Vascular disease in rheumatoid arthritis: from subclinical lesions to cardiovascular risk. Eur J Intern Med. 2009 Jul;20(4):348-54.
- Szekanecz Z, Kerekes G, Dér H, et al. Accelerated atherosclerosis in rheumatoid arthritis. Ann N Y Acad. Sci. 2007 Jun;1108:349-58.
- Roman MJ, Shanker BA, Davis A, et al. Prevalence and correlates of accelerated atherosclerosis in systemic lupus erythematosus. N Engl J Med. 2003 Dec 18;349(25):2399-406.
- Marnane M, Merwick A, Sheehan OC, et al. Carotid plaque inflammation on 18F-fluorodeoxyglucose positron emission tomography predicts early stroke recurrence. Ann Neurol. 2012 May;71(5):709-18.
- Corrado E, Rizzo M, Tantillo R, et al. Markers of inflammation and infection influence the outcome of patients with baseline asymptomatic carotid lesions: a 5-year follow-up study. Stroke. 2006 Feb;37(2):482-6.
- Ridker PM. Closing the loop on inflammation and atherothrombosis: why perform the cirt and cantos trials? Trans Am Clin Climatol Assoc. 2013;124:174-90.
- Hussein AA, Gottdiener JS, Bartz TM, et al. Inflammation and sudden cardiac death in a community-based population of older adults: The Cardiovascular Health Study. Heart Rhythm. 2013 Oct;10(10):1425-32.
- Vogel RA, Corretti MC, Plotnick GD. Effect of a single high-fat meal on endothelial function in healthy subjects. Am J Cardiol. 1997 Feb 1;79(3):350-4.
- Gerber RT, Holemans K, O’Brien-Coker I, et al. Cholesterol-independent endothelial dysfunction in virgin and pregnant rats fed a diet high in saturated fat. J Physiol. 1999 Jun 1;517 ( Pt 2):607-16.
- Wascher TC, Schmoelzer I, Wiegratz A, et al. Reduction of postchallenge hyperglycaemia prevents acute endothelial dysfunction in subjects with impaired glucose tolerance. Eur J Clin Invest. 2005 Sep;35(9):551-7.
- Piconi L, Quagliaro L, Assaloni R, et al. Constant and intermittent high glucose enhances endothelial cell apoptosis through mitochondrial superoxide overproduction. Diabetes Metab Res Rev. 2006 May-Jun;22(3):198-203.
- Newby DE, McLeod AL, Uren NG, et al. Impaired coronary tissue plasminogen activator release is associated with coronary atherosclerosis and cigarette smoking: direct link between endothelial dysfunction and atherothrombosis. Circulation. 2001 Apr 17;103(15):1936-41.
- Zhang S, Day I, Ye S. Nicotine induced changes in gene expression by human coronary artery endothelial cells. Atherosclerosis. 2001 Feb 1;154(2):277-83.
- Available at: http://www.strokeassociation.org/STROKEORG/LifeAfterStroke/HealthyLivingAfterStroke/ UnderstandingRiskyConditions/Atherosclerosis-and-Stroke_UCM_310426_Article.jsp. Accessed January 13, 2014.
- Sena CM, Pereira AM, Seiça R. Endothelial dysfunction - a major mediator of diabetic vascular disease. Biochim Biophys Acta. 2013 Dec;1832(12):2216-31.
- Grassi D, Desideri G, Ferri C. Protective effects of dark chocolate on endothelial function and diabetes. Curr Opin Clin Nutr Metab Care. 2013 Nov;16(6):662-8.
- Hoffmann J, Haendeler J, Aicher A, et al. Aging enhances the sensitivity of endothelial cells toward apoptotic stimuli: important role of nitric oxide. Circ Res. 2001 Oct 12;89(8):709-15.
- Goettsch W, Lattmann T, Amann K, et al. Increased expression of endothelin-1 and inducible nitric oxide synthase isoform II in aging arteries in vivo: implications for atherosclerosis. Biochem Biophys Res Commun. 2001 Jan 26;280(3):908-13.
- de Nigris F, Williams-Ignarro S, Botti C, Sica V, Ignarro LJ, Napoli C. Pomegranate juice reduces oxidized low-density lipoprotein downregulation of endothelial nitric oxide synthase in human coronary endothelial cells. Nitric Oxide. 2006 Nov;15(3):259-63.
- Ignarro LJ, Byrns RE, Sumi D, de Nigris F, Napoli C. Pomegranate juice protects nitric oxide against oxidative destruction and enhances the biological actions of nitric oxide. Nitric Oxide. 2006 Sep;15(2):93-102.
- Kelishadi R, Gidding SS, Hashemi M, Hashemipour M, Zakerameli A, Poursafa P. Acute and long term effects of grape and pomegranate juice consumption on endothelial dysfunction in pediatric metabolic syndrome. J Res Med Sci. 2011 Mar;16(3):245-53.
- Potenza MA, Marasciulo FL, Tarquinio M, et al. EGCG, a green tea polyphenol, improves endothelial function and insulin sensitivity, reduces blood pressure, and protects against myocardial I/R injury in SHR. Am J Physiol Endocrinol Metab. 2007 May;292(5):E1378-87.
- Kim JA, Formoso G, Li Y, et al. Epigallocatechin gallate, a green tea polyphenol, mediates NO-dependent vasodilation using signaling pathways in vascular endothelium requiring reactive oxygen species and Fyn. J Biol Chem. 2007 May 4;282(18):13736-45.
- Lorenz M, Wessler S, Follmann E, et al. A constituent of green tea, epigallocatechin-3-gallate, activates endothelial nitric oxide synthase by a phosphatidylinositol-3-OH-kinase-, cAMP-dependent protein kinase-, and Akt-dependent pathway and leads to endothelial-dependent vasorelaxation. J Biol Chem. 2004 Feb 13;279(7):6190-5.
- Takizawa Y, Kosuge Y, Awaji H, et al. Up-regulation of endothelial nitric oxide synthase (eNOS), silent mating type information regulation 2 homologue 1 (SIRT1) and autophagy-related genes by repeated treatments with resveratrol in human umbilical vein endothelial cells. Br J Nutr. 2013 Dec;110(12):2150-5.
- Caimi G, Carollo C, Lo PR. Wine and endothelial function. Drugs Exp Clin Res. 2003 29(5-6):235-42.
- van de Wiel A. Nutrition and health—favorable effect of wine and wine flavonoids on cardiovascular diseases. Ned Tijdschr Geneeskd. 2002 Dec 21;146(51):2466-9.
- Gresele P, Pignatelli P, Guglielmini G, et al. Resveratrol, at concentrations attainable with moderate wine consumption, stimulates human platelet nitric oxide production. J Nutr. 2008 Sep;138(9):1602-8.
- Freedman JE, Parker C 3rd, Li L, et al. Select flavonoids and whole juice from purple grapes inhibit platelet function and enhance nitric oxide release. Circulation. 2001 Jun 12;103(23):2792-8.
- Esper RJ, Vilariño JO, Machado RA, Paragano A. Endothelial dysfunction in normal and abnormal glucose metabolism. Adv Cardiol. 2008 45:17-43.
- Rodriguez CJ, Miyake Y, Grahame-Clarke C, et al. Relation of plasma glucose and endothelial function in a population-based multiethnic sample of subjects without diabetes mellitus. Am J Cardiol. 2005 Nov 1;96(9):1273-7.
- Williams SB, Goldfine AB, Timimi FK, et al. Acute hyperglycemia attenuates endothelium-dependent vasodilation in humans in vivo. Circulation. 1998 May 5;97(17):1695-701.
- Stochmal E, Szurkowska M, Czarnecka D, et al. Association of coronary atherosclerosis with insulin resistance in patients with impaired glucose tolerance. Acta Cardiol. 2005 Jun;60(3):325-31.
- Karrowni W, Li Y, Jones PG, et al. Insulin resistance is associated with significant clinical atherosclerosis in nondiabetic patients with acute myocardial infarction. Arterioscler Thromb Vasc Biol. 2013 Sep;33(9):2245-51.
- Gage MC, Yuldasheva NY, Viswambharan H, et al. Endothelium-specific insulin resistance leads to accelerated atherosclerosis in areas with disturbed flow patterns: a role for reactive oxygen species. Atherosclerosis. 2013 Sep;230(1):131-9.
- Jagla A, Schrezenmeir J. Postprandial triglycerides and endothelial function. Exp Clin Endocrinol Diabetes. 2001 109(4):S533-47.
- Sokup A, Góralczyk B, Góralczyk K, Rość D. Triglycerides as an early pathophysiological marker of endothelial dysfunction in nondiabetic women with a previous history of gestational diabetes. Acta Obstet Gynecol Scand. 2012 Feb;91(2):182-8.
- Toma L, Stancu CS, Botez GM, Sima AV, Simionescu M. Irreversibly glycated LDL induce oxidative and inflammatory state in human endothelial cells; added effect of high glucose. Biochem Biophys Res Commun. 2009 Dec 18;390(3):877-82.
- De CR, Lenzi S. The role of LDL in the origin and progression of atherosclerosis: pathobiological concepts on the origin and development of atherosclerotic lesions and the role of the endothelium. G Ital Cardiol. 1998 Feb;28(2):158-67.
- Chen G, Qin XP, Lin J, Wang JJ, Zhou N, Li J. Minimally modified LDL induced impairment of endothelium-dependent relaxation in mesenteric arteries of mice. Yao Xue Xue Bao. 2013 Nov;48(11):1657-64.
- Dardik R, Varon D, Tamarin I, et al. Homocysteine and oxidized low density lipoprotein enhanced platelet adhesion to endothelial cells under flow conditions: distinct mechanisms of thrombogenic modulation. Thromb Haemost. 2000 Feb;83(2):338-44.
- Hassan A, Hunt BJ, O’Sullivan M, et al. Homocysteine is a risk factor for cerebral small vessel disease, acting via endothelial dysfunction. Brain . 2004 Jan;127(Pt 1):212-9.
- Woo KS, Chook P, Lolin YI, et al. Hyperhomocyst(e)inemia is a risk factor for arterial endothelial dysfunction in humans. Circulation. 1997 Oct 21;96(8):2542-4.
- Pasceri V, Willerson JT, Yeh ET. Direct proinflammatory effect of C-reactive protein on human endothelial cells. Circulation. 2000 Oct 31;102(18):2165-8.
- Available at: http://dvr.sagepub.com/content/10/6/550.abstract. Accessed February 20, 2014.
- Schalkwijk CG1, Poland DC, van Dijk W, et al. Plasma concentration of C-reactive protein is increased in type I diabetic patients without clinical macroangiopathy and correlates with markers of endothelial dysfunction: evidence for chronic inflammation. Diabetologia. 1999 Mar;42(3):351-7.
- Silva BR, Pernomian L, Bendhack LM. Contribution of oxidative stress to endothelial dysfunction in hypertension. Front Physiol. 2012 Dec 5;3:441.
- Hadi HA, Carr CS, Al Suwaidi J. Endothelial dysfunction: cardiovascular risk factors, therapy, and outcome. Vasc Health Risk Manag. 2005;1(3):183-98.
- Chrissobolis S, Miller AA, Drummond GR, Kemp-Harper BK, Sobey CG. Oxidative stress and endothelial dysfunction in cerebrovascular disease. Front Biosci (Landmark Ed). 2011 Jan 1;16:1733-45.
- Toikka JO, Ahotupa M, Viikari JS, et al. Constantly low HDL-cholesterol concentration relates to endothelial dysfunction and increased in vivo LDL-oxidation in healthy young men. Atherosclerosis. 1999 Nov 1;147(1):133-8.
- Campbell S, Genest J. HDL-C: clinical equipoise and vascular endothelial function. Expert Rev Cardiovasc Ther. 2013 Mar;11(3):343-53.
- Calabresi L, Gomaraschi M, Franceschini G. Endothelial protection by high-densitylipoproteins: from bench to bedside. Arterioscler Thromb Vasc Biol. 2003 Oct 1;23(10):1724-31.
- Ong PJ, Patrizi G, Chong WC, Webb CM, Hayward CS, Collins P. Testosterone enhances flow-mediated brachial artery reactivity in men with coronary artery disease. J Cardiol. 2000 Jan 15;85(2):269-72.
- Jones RD, Nettleship JE, Kapoor D, Jones HT, Channer KS. Testosterone and atherosclerosis in aging men: purported association and clinical implications. Am J Cardiovasc Drugs. 2005 5(3):141-54.
- Bełtowski J. Protein homocysteinylation: a new mechanism of atherogenesis? Postepy Hig Med Dosw (Online). 2005 59:392-404.
- Liao D, Tan H, Hui R, et al. Hyperhomocysteinemia decreases circulating high-density lipoprotein by inhibiting apolipoprotein A-I Protein synthesis and enhancing HDL cholesterol clearance. Circ Res. 2006 Sep 15;99(6):598-606.
- McDowell IF, Lang D. Homocysteine and endothelial dysfunction: a link with cardiovascular disease. J Nutr. 2000 Feb;130(2S Suppl):369S-372S.
- Jacobsen DW, Catanescu O, Dibello PM, Barbato JC. Molecular targeting by homocysteine: a mechanism for vascular pathogenesis. Clin Chem Lab Med. 2005 43(10):1076-83.
- Sauls DL, Wolberg AS, Hoffman M. Elevated plasma homocysteine leads to alterations in fibrin clot structure and stability: implications for the mechanism of thrombosis in hyperhomocysteinemia. J Thromb Haemost. 2003 Feb;1(2):300-6.
- Available at: https://www.lifeextension.com/magazine. Accessed January 13, 2014.
- Available at: https://www.lifeextension.com/magazine. Accessed January 13, 2014.
- Available at: https://www.lifeextension.com/magazine/2006/6/report_doctors. Accessed January 13, 2014.
- Available at: https://www.lifeextension.com/magazine. Accessed January 13, 2014.
- Available at: https://www.lifeextension.com/magazine/2005/4/awsi. Accessed January 13, 2014.
- Celermajer DS, Sorensen K, Ryalls M, et al. Impaired endothelial function occurs in the systemic arteries of children with homozygous homocystinuria but not in their heterozygous parents. J Am Coll Cardiol. 1993 Sep;22(3):854-8.
- Maron BA, Loscalzo J. The treatment of hyperhomocysteinemia. Annu Rev Med. 2009;60:39-54.
- Moustapha A, Robinson K. Homocysteine: an emerging age-related cardiovascular risk factor. Geriatrics. 1999 Apr;54(4):41,44-6,49-51.
- Xiao Y, Zhang Y, Wang M, Li X, Xia M, Ling W. Dietary protein and plasma total homocysteine, cysteine concentrations in coronary angiographic subjects. Nutr J. 2013 Nov 7;12(1):144.
- O’Callaghan P, Meleady R, Fitzgerald T, Graham I. Smoking and plasma homocysteine. Eur Heart J. 2002 Oct;23(20):1580-6.
- Hak AE, Polderman KH, Westendorp IC, et al. Increased plasma homocysteine after menopause. Atherosclerosis. 2000 Mar;149(1):163-8.
- Dankner R, Chetrit A, Lubin F, Sela BA. Life-style habits and homocysteine levels in an elderly population. Aging Clin Exp Res. 2004 Dec;16(6):437-42.
- Refsum H1, Nurk E, Smith AD, et al. The Hordaland Homocysteine Study: a community-based study of homocysteine, its determinants, and associations with disease. J Nutr. 2006 Jun;136(6 Suppl):1731S-1740S.
- Saw SM, Yuan JM, Ong CN, et al. Genetic, dietary, and other lifestyle determinants of plasma homocysteine concentrations in middle-aged and older Chinese men and women in Singapore. Am J Clin Nutr. 2001 Feb;73(2):232-9.
- de la Torre JC. Critical threshold cerebral hypoperfusion causes Alzheimer’s disease? Acta Neuropathol. 1999 Jul;98(1):1-8.
- Kim HA, Miller AA, Drummond GR, et al. Vascular cognitive impairment and Alzheimer’s disease: role of cerebral hypoperfusion and oxidative stress. Naunyn Schmiedebergs Arch Pharmacol. 2012 Oct;385(10):953-9.
- Nishimura T, Hashikawa K, Fukuyama H, et al. Decreased cerebral blood flow and prognosis of Alzheimer’s disease. Ann Nucl Med. 2007 Jan;21(1):15-23.
- Hooshmand B, Polvikoski T, Kivipelto M, et al. Plasma homocysteine, Alzheimer and cerebrovascular pathology: a population-based autopsy study. Brain. 2013 Sep;136(Pt 9):2707-16.
- Grueter BE, Schulz UG. Age-related cerebral white matter disease (leukoaraiosis): a review. Postgrad Med J. 2012 Feb;88(1036):79-87.
- Smith AD, Smith SM, de Jager CA, et al. Homocysteine-lowering by B vitamins slows the rate of accelerated brain atrophy in mild cognitive impairment: a randomized controlled trial. PLoS One. 2010 Sep 8;5(9):e12244.
- Waśkiewicz A, Sygnowska E, Broda G. Dietary intake of vitamins B6, B12 and folate in relation to homocysteine serum concentration in the adult Polish population - WOBASZ Project. Kardiol Pol. 2010 Mar;68(3):275-82.
- Lewerin C, Nilsson-Ehle H, Matousek M, Lindstedt G, Steen B. Reduction of plasma homocysteine and serum methylmalonate concentrations in apparently healthy elderly subjects after treatment with folic acid, vitamin B12 and vitamin B6: a randomised trial. Eur J Clin Nutr. 2003 Nov;57(11):1426-36.
- Schnyder G, Roffi M, Flammer Y, Pin R, Hess OM. Effect of homocysteine-lowering therapy with folic acid, vitamin B12, and vitamin B6 on clinical outcome after percutaneous coronary intervention: the Swiss Heart study: a randomized controlled trial. JAMA. 2002 Aug 28;288(8):973-9.
- Chen RY, Wittert GA, Andrews GR. Relative androgen deficiency in relation to obesity and metabolic status in older men. Diabetes Obes Metab. 2006 Jul;8(4):429-35.
- Abate N, Haffner SM, Garg A, Peshock RM, Grundy SM. Sex steroid hormones, upper body obesity, and insulin resistance. J Clin Endocrinol Metab. 2002 Oct;87(10):4522-7.
- Grossmann M, Thomas MC, Panagiotopoulos S, et al. Low testosterone levels are common and associated with insulin resistance in men with diabetes. J Clin Endocrinol Metab. 2008 May;93(5):1834-40.
- Traish AM, Saad F, Guay A. The dark side of testosterone deficiency: II. Type 2 diabetes and insulin resistance. J Androl. 2009 Jan-Feb;30(1):23-32.
- Hak AE, Witteman JC, de Jong FH, et al. Low levels of endogenous androgens increase the risk of atherosclerosis in elderly men: the Rotterdam study. J Clin Endocrinol Metab. 2002 Aug;87(8):3632-9.
- Jones RD, Nettleship JE, Kapoor D, Jones HT, Channer KS. Testosterone and atherosclerosis in aging men: purported association and clinical implications. Am J Cardiovasc Drugs. 2005 5(3):141-54.
- Ohlsson C, Barrett-Connor E, Bhasin S, et al. High serum testosterone is associated with reduced risk of cardiovascular events in elderly men. J Am Coll Cardiol. 2011 Oct 11;58(16):1674-81.
- Ruige JB, Ouwens DM, Kaufman JM. Beneficial and adverse effects of testosterone on the cardiovascular system in men. J Clin Endocrinol Metab. 2013 Nov;98(11):4300-10.
- Traish AM, Haider A, Doros G, Saad F. Long-term testosterone therapy in hypogonadal men ameliorates elements of the metabolic syndrome: an observational, long-term registry study. Int J Clin Pract. 2013 Oct 15.
- Available at: http://www.medicinenet.com/metabolic_syndrome/article.htm. Accessed January 13, 2014.
- Tan RS, Salazar JA. Risks of testosterone replacement therapy in ageing men. Expert Opin Drug Saf. 2004 Nov;3(6):599-606.
- Available at: http://www.cdc.gov/media/dpk/2013/dpk-vs-heart-disease.html. Accessed January 13, 2014.
- Available at: http://www.cbsnews.com/8301-250_162-57597162/george-w-bush-undergoes-heart-procedure. Accessed Jan. 13, 2014.
- Available at: https://www.lifeextension.com/magazine/2006/5/awsi. Accessed January 13, 2014.
- Available at: https://www.lifeextension.com/protocols#risk. Accessed January 13, 2014.
- Available at: https://www.lifeextension.com/magazine/2007/5/awsi. Accessed January 13, 2014.
- Available at: http://web2.airmail.net/uthman/pres_longev.html. Accessed February 21, 2014.
- Available at: >http://starship.python.net/crew/manus/presidents/faq/causes.html. Accessed February 21, 2014.
- Available at: http://usatoday30.usatoday.com/news/nation/2004-09-05-clinton-bypass_x.htm. Accessed January 13, 2014.
- Available at: http://www.nytimes.com/2005/03/09/national/09surgery.html?_r=0. Accessed January 13, 2014.
- Available at: http://www.buffalohearthealth.com/?p=4219. Accessed January 13, 2014.
- Available at: http://online.wsj.com/news/articles/sb10001424052702304066404579125204086074282. Accessed January 13, 2014.
- Available at: http://www.who.int/mediacentre/factsheets/fs310/en/index2.html. Accessed January 13, 2014.
- Cheney D and Reiner J. Heart: An American Medical Odyssey. Scribner; 2013.
- Chang J, Zhang G, Zhang L, Hou YP, Liu XL, Zhang L. High admission glucose levels increase Fas apoptosis and mortality in patients with acute ST-elevation myocardial infarction: a prospective cohort study. Cardiovasc Diabetol. 2013 Nov 15;12(1):171.
- Squire IB, Nelson CP, Ng LL, Jones DR, Woods KL, Lambert PC. Prognostic value of admission blood glucose concentration and diabetes diagnosis on survival after acute myocardial infarction: results from 4702 index cases in routine practice. Clin Sci (Lond). 2010 Apr;118(8):527-35.
- Vujosevic S, Radojevic N, Belada N. Influence of admission glucose profile and hemoglobin A1c on complications of acute myocardial infarction in diabetic patients. Eur Rev Med Pharmacol Sci. 2013 May;17(9):1252-7.
- Pai JK, Cahill LE, Hu FB, Rexrode KM, Manson JE, Rimm EB. Hemoglobin a1c is associated with increased risk of incident coronary heart disease among apparently healthy, nondiabetic men and women. J Am Heart Assoc. 2013 Mar 22;2(2):e000077.
- Naito R, Miyauchi K, Ogita M, et al. Impact of admission glycemia and glycosylated hemoglobin A1c on long-term clinical outcomes of non-diabetic patients with acute coronary syndrome. J Cardiol. 2013 Sep 4.
- Available at: https://www.lifeextension.com/magazine/mag2011/jan2011_Glucose-The-Silent-Killer_01.htm. Accessed January 13, 2014.
- Available at: https://www.lifeextension.com/magazine/2013/7/blood-levels-of-insulin-and-hemoglobin-a1c-in-foundation-members. Accessed February 21, 2014.
- Available at: https://www.lifeextension.com/magazine/mag2009/may2009_Heart-Attack-Risk-Factors_01.htm. Accessed January 13, 2014.
- Tomas M, Latorre G, Senti M, Marrugat J. The antioxidant function of high density lipoproteins: a new paradigm in atherosclerosis. Rev Esp Cardiol. 2004 Jun;57(6):557-69.
- Navab M, Anantharamaiah GM, Fogelman AM. The role of high-density lipoprotein in inflammation. Trends Cardiovasc Med. 2005 May;15(4):158-61.
- Spieker LE, Ruschitzka F, Lüscher TF, Noll G. HDL and inflammation in atherosclerosis. Curr Drug Targets Immune Endocr Metabol Disord. 2004 Mar;4(1):51-7.
- Ashby DT, Rye KA, Clay MA, Vadas MA, Gamble JR, Barter PJ. Factors influencing the ability of HDL to inhibit expression of vascular cell adhesion molecule-1 in endothelial cells. Arterioscler Thromb Vasc Biol. 1998 Sep;18(9):1450-5.
- Nofer JR, Brodde MF, Kehrel BE. High-density lipoproteins, platelets and the pathogenesis of atherosclerosis. Clin Exp Pharmacol Physiol. 2010 Jul;37(7):726-35.
- Mackness MI, Durrington PN, Mackness B. The role of paraoxonase 1 activity in cardiovascular disease: potential for therapeutic intervention. Am J Cardiovasc Drugs. 2004 4(4):211-7.
- Mackness B, Durrington P, McElduff P, et al. Low paraoxonase activity predicts coronary events in the Caerphilly Prospective Study. Circulation. 2003 Jun 10;107(22):2775-9.
- Mackness M, Boullier A, Hennuyer N, et al. Paraoxonase activity is reduced by a pro-atherosclerotic diet in rabbits. Biochem Biophys Res Commun. 2000 Mar 5;269(1):232-6.
- Cakatay U, Kayali R, Uzun H. Relation of plasma protein oxidation parameters and paraoxonase activity in the ageing population. Clin Exp Med. 2008 Mar;8(1):51-7.
- Marchegiani F, Marra M, Spazzafumo L, et al. Paraoxonase activity and genotype predispose to successful aging. J Gerontol A Biol Sci Med Sci. 2006 Jun;61(6):541-6.
- Mackness B, Hine D, Liu Y, Mastorikou M, Mackness M. Paraoxonase-1 inhibits oxidised LDL-induced MCP-1 production by endothelial cells. Biochem Biophys Res Commun. 2004 Jun 4;318(3):680-3.
- Graner M, James RW, Kahri J, et al. Association of paraoxonase-1 activity and concentration with angiographic severity and extent of coronary artery disease. J Am Coll Cardiol. 2006 Jun 20;47(12):2429-35.
- Soran H, Younis NN, Charlton-Menys V, Durrington P. Variation in paraoxonase-1 activity and atherosclerosis. Curr Opin Lipidol. 2009 Aug;20(4):265-74.
- Aviram M, Rosenblat M. Pomegranate for your cardiovascular health. Rambam Maimonides Med J. 2013 Apr 30;4(2):e0013.
- Rosenblat M, Aviram M. Paraoxonases role in the prevention of cardiovascular diseases. Biofactors. 2009 Jan-Feb;35(1):98-104.
- Gouedard C, Barouki R, Morel Y. Induction of the paraoxonase-1 gene expression by resveratrol. Arterioscler Thromb Vasc Biol. 2004 Dec;24(12):2378-83.
- Do GM, Kwon EY, Kim HJ, et al. Long-term effects of resveratrol supplementation on suppression of atherogenic lesion formation and cholesterol synthesis in apo E-deficient mice. Biochem Biophys Res Commun. 2008 Sep 12;374(1):55-9.
- Costa LG, Giordano G, Furlong CE. Pharmacological and dietary modulators of paraoxonase 1 (PON1) activity and expression: the hunt goes on. Biochem Pharmacol. 2011 Feb 1;81(3):337-44.
- Aviram M, Rosenblat M, Gaitini D, et al. Pomegranate juice consumption for 3 years by patients with carotid artery stenosis reduces common carotid intima-media thickness, blood pressure and LDL oxidation. Clin Nutr. 2004 Jun;23(3):423-33.
Wellness
Specialists
1-800-226-2370 - This service is FREE
7:30 AM - 12 AM (ET) Mon-Fri | 9 AM - 12 AM (ET) Sat-Sun