Life Extension Magazine®
Newsweek® Magazine recently published an article stating that reducing homocysteine levels “has no effect on your risk of heart disease or stroke.”1 Their proclamation was based on a study published in the Journal of the American Medical Association that evaluated the impact of modest homocysteine reduction in those who had already suffered a heart attack.2 One fact that Newsweek failed to grasp is that homocysteine is involved in both the initiation and progression of atherosclerosis.3-5 It’s a shame that these two events (initiation and progression) are not better differentiated in the scientific literature, as you will learn in the following paragraphs. The subjects in the study Newsweek reported on already had a myocardial infarction (heart attack) and thus suffered severe endothelial dysfunction. Catastrophic failure of the endothelium might better describe the condition of the arteries of these study subjects. Since this study was done in the UK, where dietary choices and tobacco consumption are worse than in the US, we suspect many of these post-heart attack victims’ arterial systems were already so calcified, brittle, and occluded that it would be absurd to expect a modest reduction in homocysteine to protect against future strokes and coronary events. This study Newsweek reported on helps confirm what Life Extension® long ago stated, i.e., unless all 17 vascular disease risk factors are corrected, there may be no benefit in reducing homocysteine alone or in combination with a statin drug in healthy individuals, and certainly not those with advanced arterial disease. Comparing the effects of modest homocysteine reduction in people who have already suffered a heart attack is like saying a garden hose is useless in putting out fires because a study showed it is unable to extinguish a raging inferno.
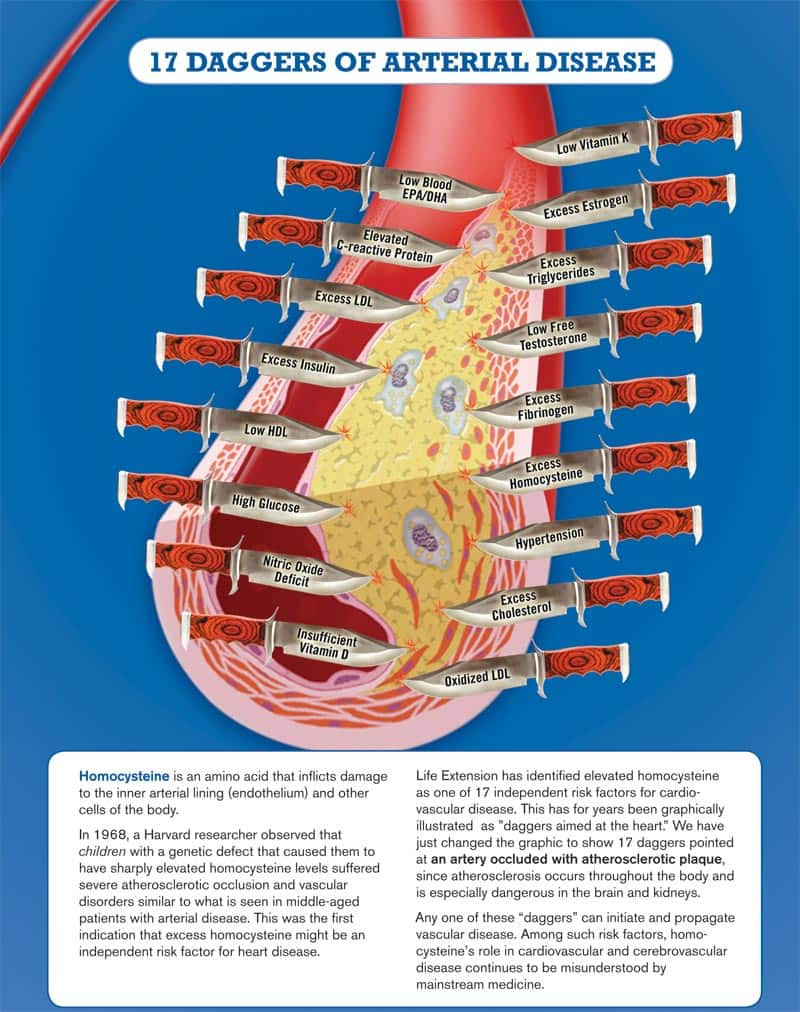
This analogy has more meaning than one might think. Those with severe pre-existing artery disease have already suffered such severe endothelial dysfunction that their arteries have become a raging oxidative and inflammatory inferno. Therapies (like homocysteine reduction) may have protected against atherosclerosis if initiated early on, but are not by themselves going to extinguish the flames raging in one’s inner arterial lining (the endothelium) after a heart attack. Fortunately there are documented approaches to reversing occlusive artery disease that can be viewed by logging on to www.lifeextension.comhttps://www.lifeextension.com/vitamins-supplements. Homocysteine reduction alone is not the solution for those with advanced atherosclerosis. Life Extension Magazine® long ago published that those with severe coronary atherosclerosis require aggressive approaches to suppress the 17 independent risk factors known to cause arterial blockage. Those who rely on the mainstream media as a source for health information are often poorly informed. One reason the media get it so wrong is that rather than performing their own scientific analysis of clinical studies, they instead act as mouthpieces for the medical establishment. If a drug company-sponsored medical journal questions the value of an alternative therapy (like homocysteine reduction), the media proclaims it to be absolute fact, instead of having scientifically-trained people evaluate the study to see if it has merit. This article exposes the many flaws of the study that the media used to attack the value of suppressing elevated homocysteine. Homocysteine is a toxic amino acid that inflicts damage to the inner arterial lining (endothelium) and other cells of the body. In 1968, a Harvard researcher observed that children with a genetic defect that caused them to have sharply elevated homocysteine levels suffered severe atherosclerotic occlusion similar to what is seen in middle-aged patients with arterial disease. This was the first indication that excess homocysteine might be an independent risk factor for heart disease. Elevated homocysteine is one of 17 independent risk factors for cardiovascular disease. For years Life Extension has graphically illustrated these risk factors as “daggers aimed at the heart.” We have changed the graphic to show 17 daggers pointed at an artery occluded with atherosclerotic plaque, as you will see on the next page. We changed this graphic because atherosclerosis adversely affects blood vessels throughout the body. Any one of these “daggers” can initiate and propagate vascular disease. Among such risk factors, homocysteine’s role in cardiovascular and cerebrovascular disease continues to be misunderstood by mainstream medicine. And it’s happened again. A widely publicized study in a medical establishment journal is being touted as showing “no benefit” for homocysteine-lowering therapy using vitamin supplementation.2 But the study design has so many flaws, and is so misguided in its fundamental purpose, as to be entirely (even dangerously) irrelevant. The study has one valuable aspect, however. It highlights the continuing failure of mainstream medicine to understand the complexities of cardiovascular disease. It also exposes a strong bias towards single-focused, drug-oriented therapies—beneficial for pharmaceutical companies, maybe, but hardly a responsible scientific approach to disease reduction. Here are the basic “findings” of this most recent misguided study. The authors acknowledge the unquestionable relationship of homocysteine, a toxic amino acid, with cardiovascular disease.6 They then seek to assess the effects of reducing homocysteine levels, using folic acid and vitamin B12 supplements, on cardiovascular and other health outcomes. And they study an enormous population (more than 12,000 people). Sounds good so far. But in a typical “horse-is-out-of-the-barn” fashion, the study includes only people who are survivors of at least one heart attack! The main outcome measure to determine success or failure of homocysteine-lowering therapy was any major vascular event, defined as heart attack, bypass surgery or stent placement, stroke, or death from heart attack or stroke. The researchers found no significant differences in any of these disastrous outcomes between people who’d lowered their homocysteine levels and those who hadn’t. But since 100% of the subjects in this study had already suffered a major heart attack, we know a priori that their cardiovascular systems were in advanced stages of malfunction. Yet the researchers concluded that “Substantial long-term reductions in blood homocysteine levels with folic acid and vitamin B12 supplementation did not have beneficial effects on vascular outcomes.”2 Sadly, this is not the first time that a prestigious journal has published such a flawed document and claimed it was good science. Two studies published in the New England Journal of Medicine in the middle of the last decade made similar claims.7,8 One studied people with existing vascular disease or diabetes,8 and the other studied people who had suffered a heart attack.7 These aren’t the only errors in these studies. And they aren’t benign errors. Suggesting that homocysteine-lowering isn’t valid prevention for cardiovascular disease is a potentially grave and dangerous mistake. It’s one that ignores most of what we actually know about the multifactorial causes of heart attacks and strokes. It’s one that doesn’t apply to the vast majority of people who haven’t yet had a catastrophic event. And it’s one that could discourage millions of Americans from adopting a powerful therapy that can contribute meaningfully to risk reduction. Let’s look harder at the most recent study, and dissect its multiple flaws. That way, readers will be able to make informed decisions about their own health. Inadequate Homocysteine LoweringThe recent JAMA study provided 2 mg folic acid plus 1 mg vitamin B12 daily, which are reasonable starting doses.2 But the researchers made an astonishing oversimplification based on 15-year-old data. They assumed that simply lowering homocysteine levels by 3 micromoles per liter (μmol/L) would create a 20-25% lower risk of cardiovascular events.2,9 In other words, no matter what your baseline homocysteine level was, the researchers expected to see a linear decrease in risk for each 3 μmol/L drop in homocysteine. That’s just not how most biological systems work—there’s typically a threshold level above which a given factor increases risk, and below which risk accumulates more slowly. That put the JAMA study at risk for failing to detect any effect in the first place. Next, the amount of actual lowering of homocysteine levels was inadequate. Baseline homocysteine levels were 13.5 μmol/L, in the range we know is associated with increased risk of cardiovascular disease and death.6,10 That’s hardly surprising, since all subjects had already had a heart attack. But the study protocol only brought the average homocysteine level down to 9.8.2 That’s still in the range known to produce a 31% increase in stroke risk, and at least a 9% increase in overall risk of dying from cardiovascular disease!6,10 Worse, in their actual analysis, the JAMA authors lumped all homocysteine levels less than 11 μmol/L into their lowest category. That means they included people with homocysteine levels of 7-8 right along with people who had levels as high as 10.9 into one group.2 So it’s hardly surprising that their analysis showed no effect. Life Extension long ago advocated that members take aggressive steps to keep homocysteine levels below 7-8 µmol/L.11-13 The rationale was based on an extrapolation of the existing published studies relating to homocysteine blood levels and heart attack risk. So the new JAMA study is incapable of demonstrating any effect of lowering homocysteine into the recommended range for otherwise healthy people—it just wasn’t designed to do so.
Baseline Homocysteine Levels—Not High Enough in the First Place?We’ve seen that patients in the JAMA study were sick—they had to have major cardiovascular disease just to get into the study. Why weren’t their homocysteine levels considerably higher (many studies find levels of 30-50 μmol/L)?14 This is where the researchers’ third major error is evident. Cardiovascular disease is the result of many different, interacting risk factors (see the “17 Daggers” Life Extension Foundation® has identified on page 2). People who have experienced actual negative outcomes such as heart attacks have obviously been exposed to many of those risk factors acting in concert over a lifetime. It’s naive to expect that simply reducing one risk factor, and only modestly at that, would produce a measurable reduction in risk. That’s especially true for people whose bodies are already rife with vascular damage. Life Extension advocates an across-the-board approach to risk reduction, one that addresses all of the known risk factors for cardiovascular disease. It’s one centered on the fundamental problem of endothelial dysfunction. Other Cardiovascular Risk Factors Not ConsideredA glance at the baseline characteristics of patients in the JAMA study reveals a fourth substantial error. As with previous “no effect” studies, this most recent investigation included people with substantial additional risk factors for cardiovascular disease. Again that’s hardly surprising in a study that chose to examine only subjects with a history of heart attack. For example, in addition to heart attacks, 9% of patients in this study had other vascular complications and an additional 11% had known diabetes.2 Sixty-eight percent had elevated LDL cholesterol, and 42% had pre-existing hypertension. Sixty-five percent were ex-smokers, while 12% of subjects were actually still smoking at the time of the study. So a whopping 77% of subjects were vulnerable to the lifelong effects of one of the highest-risk habits known to medicine! No other risk factors, out of the myriad that are known markers for cardiovascular disease or the conditions leading up to it, were measured. That means no C-reactive protein (CRP), no determinations of insulin sensitivity or the presence of advanced glycation end-products (AGEs), and no hormonal determinations. Life Extension advocates an across-the-board approach to risk reduction, one that addresses all of the known risk factors for cardiovascular disease.
Finally (and typically), no other integrated therapies or lifestyle changes were provided, other than a standard dose of simvastatin, a cholesterol-lowering medication.2 In other words, this was a classic mainstream medicine study looking at a single intervention in isolation. The study subjects never really had a chance. A Fundamental Lack of Understanding of Endothelial DysfunctionThe errors in conception and design of the most recent JAMA study are unfortunately typical not only of modern researchers, but also of many practicing physicians. As a result, patients are often missing the benefits of some breakthroughs in what we know about cardiovascular disease. Astonishingly, the phrase “endothelial dysfunction” (and even the single word “endothelium”) appears nowhere in the entire article! Yet endothelial dysfunction is at the core of our modern understanding of atherosclerosis.
The endothelium is the single cell layer lining arterial walls. It is a potent tissue in its own right, not only protecting the thick muscular layer of the artery from damage, but also subtly detecting and transmitting information about the state of the bloodstream to the artery as a whole. The earliest event in the cascade leading to cardiovascular disease is endothelial damage. Homocysteine is one of the many common blood-borne substances that damage endothelial tissue, exposing it to oxidant and ultimately inflammatory injury.15-17 The damage is exacerbated throughout life by smoking, poor diet, obesity, and nutrient deficiencies.18-23 Homocysteine is particularly dangerous because it can be one of the earliest (and hence one of the most preventable) causes of endothelial damage—and it does so by a host of interlocking mechanisms. Homocysteine is a potent excitatory neurotransmitter that drives oxidative stress and increases death of endothelial cells through apoptosis.15 These events lead to inflammation, an influx of fat-laden inflammatory cells, and eventually to the arterial blockage that we recognize as cardiovascular disease. And that explains why this most recent JAMA study, like its predecessors, was doomed to fail. | ||||||




Asking Too Much and Doing Too LittleFundamentally, these clinical studies were asking too much and doing too little. They produced only moderate reductions in homocysteine levels in people already gravely ill with cardiovascular disease. They add nothing to what we already know about the role of homocysteine in otherwise healthy people—people who still have a chance to make important changes in all of the known cardiovascular risk factors. It’s vital to make those changes early, before damage accumulates, and to make them in as many risk areas as possible. Homocysteine reduction is one such area, and we have solid evidence that an early start aimed at reducing levels substantially can make a big difference. Traditional wisdom holds that endothelial dysfunction only begins to occur in otherwise healthy people when their homocysteine levels get above the upper limit of “normal,” 15 μmol/L.24 But we’ve known for more than a decade that even small increments in homocysteine levels—within the “normal” range—produce immediate and dangerous disruptions of endothelial function. In a remarkable study in 1999, British researchers fed healthy young adults several different diets, two of which contained amino acid precursors of homocysteine, and one that was free of such molecules.25 At baseline, volunteers had mean homocysteine levels of 9.5 μmol/L. Both the homocysteine precursor-containing diets induced an immediate rise in plasma homocysteine, but only to the 11-12 μmol/L range. Nonetheless, there was an immediate decrease in flow-mediated dilation, a sensitive measure of endothelial function. The control diet had no effect. It’s hard to ask for more direct proof that small homocysteine elevations produce meaningful reductions in endothelial function and lay the foundation for atherosclerosis.
Doomed from the OutsetArmed with a realistic understanding of how homocysteine levels relate to cardiovascular risk, it is easy to see why the recent JAMA study failed to show any impact of minor homocysteine lowering on people with major heart disease. Reducing homocysteine by a few points, at the lower end of the scale, in people with pre-existing severe arterial damage (severe enough to have already had a heart attack), could not possibly be expected to have an impact. The approach taken by mainstream physicians in studies like the JAMA report are tragically typical of their general strategy. That can be summed up as, “Find a single problem, focus on it and it alone, and judge success or failure by whether changing just the one factor makes a difference.” That’s a great way to sell drugs, of course—one drug per problem adds up to tremendous revenue. But it is a poor way to manage the complexities of cardiovascular disease, for which we can identify no fewer than 17 deadly risk factors (and perhaps many more).
The Bottom LineIt’s naive to claim that a single therapy can have an impact on a complex, multifaceted problem like cardiovascular disease. Homocysteine-lowering, by itself, will not prevent a heart attack. By the same token, however, throwing out several decades of solid evidence that homocysteine-lowering can substantially reduce the risk of cardiovascular disease is worse than naive—it’s downright dangerous. Studies like the JAMA report will no doubt continue to appear, and will continue to be misrepresented as “evidence” that close attention to homocysteine levels is unnecessary. It is in the financial interests of mainstream cardiology to deceive the public into believing the only way of treating heart disease is with bypass surgery, stents, and drugs.
A plethora of published data, however, reveals that aging humans can successfully circumvent the lethal atherosclerotic process and in many cases reverse it. It all starts with comprehensive blood testing. The medical establishment charges around $1,000 for the wide-ranging blood tests needed to assess coronary risk markers. As a Life Extension member, you can obtain the same tests for only $269. When you place your blood test order, we send you a requisition form along with a listing of blood-drawing stations in your area. You can normally walk in during regular business hours for a convenient blood draw. The sidebar below describes the comprehensive Male and/or Female Blood Test Panels that all health conscious individuals should have done at least once a year. They can be ordered by calling 1-800-208-3444 (24 hours a day). If you have any questions on the scientific content of this article, please call a Life Extension® Health Advisor at 1-866-864-3027.
| ||||||||||||||||||||
| References | ||||||||||||||||||||
| 1. Available at: http://www.newsweek.com/2010/06/22/observe-and-report.html. Accessed September 7, 2010. 2. SEARCH Collaborative Group, Armitage JM, Bowman L, et al. Effects of homocysteine-lowering with folic acid plus vitamin B12 vs placebo on mortality and major morbidity in myocardial infarction survivors: a randomized trial. JAMA. 2010 Jun 23;303(24):2486-94. 3. Geisel J, Jodden V, Obeid R, Knapp JP, Bodis M, Herrmann W. Stimulatory effect of homocysteine on interleukin-8 expression in human endothelial cells. Clin Chem Lab Med. 2003 Aug;41(8):1045-8. 4. Poddar R, Sivasubramanian N, DiBello PM, Robinson K, Jacobsen DW. Homocysteine induces expression and secretion of monocyte chemoattractant protein-1 and interleukin-8 in human aortic endothelial cells: implications for vascular disease. Circulation. 2001 Jun 5;103(22):2717-23. 5. Su SJ, Huang LW, Pai LS, Liu HW, Chang KL. Homocysteine at pathophysiologic concentrations activates human monocyte and induces cytokine expression and inhibits macrophage migration inhibitory factor expression. Nutrition. 2005 Oct;21(10):994-1002. 6. Nygard O, Nordrehaug JE, Refsum H, Ueland PM, Farstad M, Vollset SE. Plasma homocysteine levels and mortality in patients with coronary artery disease. N Engl J Med. 1997 Jul 24;337(4):230-6. 7. Bonaa KH, Njolstad I, Ueland PM, et al. Homocysteine lowering and cardiovascular events after acute myocardial infarction. N Engl J Med. 2006 Apr 13;354(15):1578-88. 8. Lonn E, Yusuf S, Arnold MJ, et al. Homocysteine lowering with folic acid and B vitamins in vascular disease. N Engl J Med. 2006 Apr 13;354(15):1567-77. 9. Boushey CJ, Beresford SA, Omenn GS, Motulsky AG. A quantitative assessment of plasma homocysteine as a risk factor for vascular disease. Probable benefits of increasing folic acid intakes. JAMA. 1995 Oct 4;274(13):1049-57. 10. Iso H, Moriyama Y, Sato S, et al. Serum total homocysteine concentrations and risk of stroke and its subtypes in Japanese. Circulation. 2004 Jun 8;109(22):2766-72. 11. A lethal misconception. Life Extension Magazine®. 1999 Mar;5(3). 12. Baron P. A comprehensive guide to complete blood testing. Life Extension Magazine®. 2004 May;10(5):51-71. 13. Faloon W. Startling findings about homocysteine. Life Extension Magazine®. 2003 Nov;9(11):11-6. 14. Bazzano LA, Reynolds K, Holder KN, He J. Effect of folic acid supplementation on risk of cardiovascular diseases: a meta-analysis of randomized controlled trials. JAMA. 2006 Dec 13;296(22):2720-6. 15. McCully KS. Chemical pathology of homocysteine. IV. Excitotoxicity, oxidative stress, endothelial dysfunction, and inflammation. Ann Clin Lab Sci. 2009 Summer;39(3):219-32. 16. Vizzardi E, Bonadei I, Zanini G, Fiorina C, Raddino R, Dei Cas L. Homocysteine: a casual link with heart failure? Minerva Med. 2009 Oct;100(5):421-7. 17. Park CS, Ihm SH, Yoo KD, et al. Relation between C-reactive protein, homocysteine levels, fibrinogen, and lipoprotein levels and leukocyte and platelet counts, and 10-year risk for cardiovascular disease among healthy adults in the USA. Am J Cardiol. 2010 May 1;105(9):1284-8. 18. Haynes WG. Hyperhomocysteinemia, vascular function and atherosclerosis: effects of vitamins. Cardiovasc Drugs Ther. 2002 Sep;16(5):391-9. 19. Grassi D, Desideri G, Ferri L, Aggio A, Tiberti S, Ferri C. Oxidative stress and endothelial dysfunction: Say no to cigarette smoking! Curr Pharm Des. 2010 Jun 15. 20. Puntmann VO, Taylor PC, Mayr M. Coupling vascular and myocardial inflammatory injury into a common phenotype of cardiovascular dysfunction: Systemic inflammation and aging - a mini-review. Gerontology. 2010 Jun 11. 21. Sucharda P. Obesity and atherosclerosis--what’s the link? Vnitr Lek. 2010 Apr;56(4):289-91. 22. Urso C, Hopps E, Caimi G. Adhesion molecules and diabetes mellitus. Clin Ter. 2010 Jan-Feb;161(1):e17-24. 23. Wang M, Monticone RE, Lakatta EG. Arterial aging: a journey into subclinical arterial disease. Curr Opin Nephrol Hypertens. 2010 Mar;19(2):201-7. 24. Bellamy MF, McDowell IF, Ramsey MW, Brownlee M, Newcombe RG, Lewis MJ. Oral folate enhances endothelial function in hyperhomocysteinaemic subjects. Eur J Clin Invest. 1999 Aug;29(8):659-62. 25. Chambers JC, Obeid OA, Kooner JS. Physiological increments in plasma homocysteine induce vascular endothelial dysfunction in normal human subjects. Arterioscler Thromb Vasc Biol. 1999 Dec;19(12):2922-7. 26. Clarke R, Armitage J. Vitamin supplements and cardiovascular risk: review of the randomized trials of homocysteine-lowering vitamin supplements. Semin Thromb Hemost. 2000;26(3):341-8. 27. Krishnaswamy K, Lakshmi AV. Role of nutritional supplementation in reducing the levels of homocysteine. J Assoc Physicians India. 2002 May;50 Suppl:36-42. 28. Schwammenthal Y, Tanne D. Homocysteine, B-vitamin supplementation, and stroke prevention: from observational to interventional trials. Lancet Neurol. 2004 Aug;3(8):493-5. 29. Hirsch S, Pia De la Maza M, Yanez P, et al. Hyperhomocysteinemia and endothelial function in young subjects: effects of vitamin supplementation. Clin Cardiol. 2002 Nov;25(11):495-501. 30. Flicker L, Vasikaran SD, Thomas J, et al. Efficacy of B vitamins in lowering homocysteine in older men: maximal effects for those with B12 deficiency and hyperhomocysteinemia. Stroke. 2006 Feb;37(2):547-9. 31. Lim HS, Heo YR. Plasma total homocysteine, folate, and vitamin B12 status in Korean adults. J Nutr Sci Vitaminol (Tokyo). 2002 Aug;48(4):290-7. 32. Yajnik CS, Lubree HG, Thuse NV, et al. Oral vitamin B12 supplementation reduces plasma total homocysteine concentration in women in India. Asia Pac J Clin Nutr. 2007;16(1):103-9. 33. Chiu YW, Chang JM, Hwang SJ, Tsai JC, Chen HC. Pharmacological dose of vitamin B12 is as effective as low-dose folinic acid in correcting hyperhomocysteinemia of hemodialysis patients. Ren Fail. 2009;31(4):278-83. 34. Azadibakhsh N, Hosseini RS, Atabak S, Nateghiyan N, Golestan B, Rad AH. Efficacy of folate and vitamin B12 in lowering homocysteine concentrations in hemodialysis patients. Saudi J Kidney Dis Transpl. 2009 Sep;20(5):779-88. | ||||||||||||||||||||




Wellness
Specialists
1-800-226-2370 - This service is FREE
7:30 AM - 12 AM (ET) Mon-Fri | 9 AM - 12 AM (ET) Sat-Sun