Life Extension Magazine®
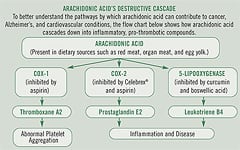
Life Extension, always at the forefront in uncovering the latest scientific and medical breakthroughs for our members, recommended aspirin therapy for cardiovascular protection long before this practice became a standard treatment by cardiologists and other doctors. Life Extension continues to closely scrutinize ongoing scientific research associated with aspirin. Recently, scientists have uncovered tantalizing evidence suggesting that aspirin may help prevent skin cancer and reduce the risk of Alzheimer's disease. The common thread linking aspirin’s beneficial effects on colorectal cancer, skin cancer, and Alzheimer's appears to be its remarkable ability to reduce excess inflammation and promote healthy blood flow. Today, medical science is confirming what Life Extension members have known for some time—that chronic inflammation underlies many of the most lethal degenerative diseases. Cells throughout the body manufacture hormone-like substances called prostaglandins, which are involved in fever, inflammation, and pain, as well as thromboxanes, which help regulate blood vessel tone, platelet aggregation, and clot formation.1,2 The fatty acid arachidonic acid is transformed into prostaglandins and thromboxanes through the action of the cyclooxygenase (COX) enzymes. Aspirin works by irreversibly disabling the COX enzymes so that they can no longer produce prosta-glandins and thromboxanes.3-5
By reducing prostaglandin and thromboxane production, aspirin decreases inflammation, pain, fever, and blood clotting. As people grow older, they commonly experience increased inflammation as well as a greater prevalence of undesirable blood-clotting tendencies. Scientists believe that increased oxidative stress and greater levels of pro-inflammatory mediators may induce these changes in aging adults.6,7 Aspirin’s demonstrated ability to reduce inflammation may play a key role in helping to counteract many of the adverse biochemical changes that accompany aging. These very same properties also make aspirin a powerful weapon against many major diseases, including cardiovascular disease and cancer.
Aspirin and Cancer PreventionLife Extension has long warned that chronic inflammation can pave the way for many deadly diseases, including cancer. Inflammation plays many roles in encouraging normal cells to become cancerous. For example, inflammation generates free radicals that can damage the genetic material responsible for regulating normal cell death and reproduction.11 While the bulk of the research examining aspirin’s effects against cancer has focused on colorectal cancer, emerging evidence indicates that aspirin may also markedly reduce the risk of cancers of the skin, breast, ovary, lung, and other organs.12 Aspirin offers protection against cancer through its effects on the COX enzymes. While the COX-1 enzyme promotes blood clotting and helps protect the stomach lining, COX-2 participates in harmful inflammation and cancer. Aspirin inhibits both types of COX enzymes, which may account for its protective effects against various cancers.12 Life Extension has long advocated the use of anti-inflammatory therapies, including natural therapeutics such as curcumin and green tea, as strategies to help prevent and fight cancer.13 Aspirin lowers skin cancer risk. A recent study out of sun-drenched Australia offers compelling evidence that aspirin use protects against skin cancer. This study found that people who regularly used aspirin and other nonsteroidal anti-inflammatory drugs (NSAIDs) were less likely to develop squamous cell carcinoma and actinic keratosis (a pre-cancerous skin condition linked to excessive sun exposure). The lead investigator reported that people who had used aspirin or other NSAIDs at least twice a week for five years reduced their risk of skin cancer by a remarkable 60%, while those who used aspirin daily for five years saw an astounding decrease of nearly 90% in their risk of developing skin cancer. The benefits from regular use of NSAIDs were evident after as little as one year of use, according to the study authors.14,15 Aspirin reduces breast cancer risk. Aspirin may offer protection against two cancers that afflict women: breast cancer and ovarian cancer. A study reported in late 2005 noted that women who used more than 100 mg of aspirin on a frequent basis (for 90 days or more) during the year prior to mammogram testing had a lower risk of breast cancer than infrequent users or non-users of aspirin.16 In 2006, researchers reported the findings of a population-based, case-controlled study of women with ovarian cancer. They noted that women who used any NSAIDs such as aspirin within the previous five years had a reduced risk of developing ovarian cancer. Their data suggests that greater use of NSAIDs correlates with a lower risk of ovarian cancer.17 Aspirin protects against colon cancer. In a double-blind study reported in 2003, researchers gave groups of more than 350 adults a daily dose of either 81 or 325 mg of aspirin, or a placebo pill, for three years. All the subjects had had colon polyps removed in the past, but were free of polyps at the study’s onset. Many colon cancers are thought to develop from polyps. After approximately three years, the subjects underwent another colonoscopy to determine how many growths were present. Subjects who took the 81-mg dose of aspirin had 19% fewer polyps than those in the placebo group. The researchers concluded that low-dose aspirin had a modest effect in reducing the incidence of potentially pre-cancerous polyps.18 Another study examined 635 patients with a history of colorectal cancer. Half took 325 mg of aspirin a day, while half took a placebo. After roughly a year, each group underwent a colonoscopy to check for polyps. The results were even more impressive: subjects in the aspirin group had a 35% lower risk of polyps than those who took placebo. In addition, it took longer for polyps to develop in the subjects who took aspirin.19 These findings suggest an important role for aspirin in preventing colon cancer. Aspirin and Alzheimer's DiseaseAlzheimer's disease not only changes people’s mental abilities, but also alters the physical appearance of their brains. In people who have Alzheimer's, the brain tissue literally shrinks.20 This condition is also marked by scattered, abnormal structures called beta-amyloid plaques and neurofibrillary tangles. In Alzheimer's disease, beta-amyloid plaques are found around the cerebral cortex, as well as in a structure deeper in the brain called the hippocampus, which plays a role in memory storage. Neurofibrillary tangles are found inside the neurons, where they can cause the neuron to have difficulty communicating with other neurons, and later to die. Although many healthy older people have some plaques and tangles in their brains, people with Alzheimer's disease have far more. Substances involved in inflammation have been found in these plaques, and scientists suspect this inflammation contributes to neuronal death.21
One potentially dangerous substance that has been found in the brains of Alzheimer's sufferers is the COX-2 enzyme. Some research has shown a link between excess COX enzymes and prostaglandins with more beta-amyloid in brains. Elevated COX-2 has also been found in hippocampal neurons of people with Alzheimer's, and has been correlated with the withering of neurons and more dense plaques in that region of the brain.22 Another theory suggests that prostaglandins produced by the COX enzymes may also increase the effects of a neurotransmitter called glutamate. Neurotransmitters such as glutamate help nerve cells communicate. If too much glutamate lingers in the space between neurons, it can overstimulate the cells, causing them to die. Researchers have proposed that inhibiting the COX enzymes and thus reducing prostaglandins could reduce the excess stimulation caused by glutamate, thus protecting cells against inflammation and neurodegenerative disease.23-25 Regular use of anti-inflammatory drugs, particularly aspirin, has been associated with a lower prevalence of Alzheimer's disease, along with improved preservation of cognitive function. For example, a meta-analysis examined the use of NSAIDs in relation to the development of Alzheimer's disease in adults over the age of 55. Individuals who regularly used anti-inflammatory drugs had a decreased risk of developing Alzheimer's, and the risk reduction increased as the duration of anti-inflammatory use lengthened. People who used the anti-inflammatory medications for 24 months, for example, had an amazing 73% reduced risk of developing Alzheimer's.26 An analysis of more than 700 individuals over the age of 80 showed that those who regularly used aspirin had a markedly lower prevalence of Alzheimer's dementia. Furthermore, this group maintained better cognitive function than those who did not use aspirin.27 | ||||||


Aspirin’s Role in Heart DiseaseLife Extension has repeatedly alerted its members to the lethal dangers of endothelial dysfunction, the key underlying factor in the progression of atherosclerosis, or hardening of the arteries. (See “Why Our Arteries Become Clogged as We Age,” Life Extension, October 2005.) Endothelial dysfunction occurs when the blood vessel linings can no longer dilate in response to demands for increased blood flow. Emerging studies indicate that aspirin may protect against heart disease in part by improving endothelial function. In a study of 14 patients with coronary atherosclerosis, aspirin helped improve the ability of blood vessels to dilate, indicating an improvement in endothelial function. This led the study authors to suggest that aspirin therapy could help improve endothelial dysfunction and inhibit the advance of atherosclerosis.28
The heart depends on its coronary arteries for the oxygen supply that fuels this most vital of organs. Coronary heart disease occurs when normal blood flow through the arteries that feed the heart is slowed or interrupted by factors such as blood clots or plaque. Preventing clots is another way that aspirin helps prevent heart attacks. By irreversibly blocking production of the clot-promoting biochemicals known as thromboxanes, aspirin prevents platelets in the blood from latching on to each other and forming a clot. A platelet has a life span of 10 days, and aspirin permanently impairs the platelet’s clotting ability.29 Aspirin helps blood flow more smoothly past any plaque that is narrowing an artery, and if a plaque ruptures, aspirin will reduce the likelihood of a clot clinging to it.30 Aspirin can also help prevent heart disease through its anti-inflammatory action. Inflammation participates in many disease processes in the body, including plaque accumulation in the arteries.31 The growth of plaque can obstruct blood flow through the arteries. If a plaque ruptures due to inflammation, it can trigger a heart attack. A 2003 meta-analysis examined aspirin’s effects on primary heart-attack prevention (that is, the prevention of first heart attacks). In more than 55,000 men and women, aspirin use was associated with a 32% reduction in the risk of having a first heart attack, and with a 15% reduction in the risk of all major vascular events.32 A study presented at the 2005 meeting of the American Heart Association reported on the lifesaving benefits of aspirin therapy. This study examined nearly 9,000 women with stable heart disease, ranging in age from 50 to 79. During more than six years of follow-up, women taking aspirin were 25% less likely to die from heart disease and 17% less likely to die from any cause. Some women took 81 mg of aspirin daily, while others took 325 mg. The study authors stated that the two doses appeared to be similarly effective, but that higher doses of aspirin are associated with a greater risk of certain side effects, such as stomach bleeding.33 A meta-analysis published in 2006 examined the effects of aspirin therapy in preventing cardiovascular events in women and men. Examining data from more than 50,000 women, investigators determined that aspirin therapy was associated with a significant 12% reduction in cardiovascular events in women. Among more than 44,000 men, aspirin therapy produced a significant 14% reduction in all cardiovascular events and an even more impressive 32% reduction in heart attacks.34 According to the US Preventive Services Task Force, aspirin’s proven benefits are reason enough for people to start using it if they have at least a 6% chance of developing coronary heart disease in the next 10 years. By contrast, the American Heart Association recommends aspirin for people whose 10-year risk of developing coronary heart disease is 10% or higher, as long they have no medical contraindications for taking the drug. A doctor can help you calculate your cardiovascular risk based on factors such as tobacco use, cholesterol, and blood pressure.35,36 You can also assess your cardiovascular risk by using online risk factor calculators available at the American Heart Association website. Life Extension strongly recommends that people who have already had a heart attack (or other episode of heart disease) discuss aspirin therapy with their doctor as part of a strategy to prevent future problems. Life Extension also suggests that people with no previous history of cardiovascular disease—but who are nevertheless at high risk for heart disease—strongly consider aspirin therapy in consultation with their personal physician. The recommended dose for preventing heart-related problems is 81-325 mg daily. Speak with your doctor about your personal needs before beginning aspirin therapy. Aspirin and Stroke: Risk vs. BenefitThe brain requires a constant supply of oxygen from freshly flowing blood to convert glucose into energy.38 During a stroke, blood flow to part of the brain is cut off, and the damage from this interruption can cause death, disability, impaired speech, and myriad other adverse effects.
The most common type of stroke—known as ischemic stroke—occurs when an artery becomes blocked, limiting blood supply to areas of the brain. This type of stroke accounts for about 80% of stroke cases. The other 20% or so are cases of hemorrhagic stroke, which is caused by a blood vessel rupturing and spilling blood into the brain. Aspirin plays vastly different roles in these two types of stroke. Aspirin helps to decrease the risk of ischemic stroke by keeping blood platelets from sticking together to form a clot, so that blood continues to flow past any narrowed spots in the arteries that feed the brain. However, some studies suggest that taking aspirin may cause a slight increase in a person’s chance of having a hemorrhagic stroke. The US Preventive Services Task Force estimates that if 1,000 people took aspirin for five years, as many as 2 would suffer a hemorrhagic stroke.39 A study published in March 2005 examined aspirin’s effects on women. Nearly 40,000 middle-aged and older women were assigned to take either placebo or 100 mg of aspirin every other day for 10 years. Women who took aspirin had a notable 24% reduced risk of ischemic stroke. In this study, however, aspirin use was associated with slightly higher risks of gastrointestinal bleeding and hemorrhagic stroke.40
Another study reported in late 2005 examined the effects of aspirin therapy in more than 50,000 women who did not have coronary heart disease. Aspirin use was associated with a 17% reduction in the risk of suffering a stroke, and a 24% reduction in the risk of ischemic stroke. In this study, aspirin use did not appear to increase the risk of hemorrhagic stroke.33 Once your risk factors for stroke—like hypertension, high cholesterol, diabetes, or smoking—start adding up, you and your doctor need to discuss aspirin therapy, particularly as you grow older and advance into age groups that bear a heavier stroke risk. If you have suffered a hemorrhagic stroke, aspirin should not be used. In general, 81-325 mg of aspirin daily is used as part of a stroke-prevention program.
ConclusionLife Extension was at the forefront in advocating aspirin use to decrease cardiovascular risk, long before the mainstream medical community finally recognized the lifesaving benefits of aspirin. Exciting new research findings support a disease-preventive benefit for aspirin in other potentially lethal conditions such as skin cancer, colon cancer, and Alzheimer's. Life Extension will continue to monitor ongoing research on aspirin and share with members important findings that are often overlooked by the mainstream medical establishment. An overlooked staple of the medicine cabinet, aspirin continues to prove its value as one of our most powerful allies in fighting the deadly diseases that accompany aging. Caution: Individuals with allergies to aspirin or other salicylates should not use aspirin. People with a history of bleeding disorders, hemorrhagic stroke, asthma, or ulcers should speak with a doctor before using aspirin. Consult a physician before using aspirin in combination with over-the-counter or prescription medications. Children and teenagers with symptoms of flu or chicken pox should not take aspirin. | ||||||
| References | ||||||
| 1. Crofford LJ. Prostaglandin biology. Gastroenterol Clin North Am. 2001 Dec;30(4):863-76. 2. Available at: http://en.wikipedia.org/wiki/Thromboxane. Accessed May 8, 2006. 3. Bayer A. Clinicians’ Guide to Aspirin. London: Arnold; 1998. 4. Norman AW, Litwack G. Hormones. 2nd ed. Burlington, MA: Academic Press; 1997. 5. Available at: http://en.wikipedia.org/wiki/ Aspirin. Accessed May 8, 2006. 6. McGeer EG, Klegeris A, McGeer PL. Inflammation, the complement system and the diseases of aging. Neurobiol Aging. 2005 Dec;26 Suppl 1:94-7. 7. Dinarello CA. Interleukin 1 and interleukin 18 as mediators of inflammation and the aging process. Am J Clin Nutr. 2006 Feb;83(2):447S-55S. 8. Roberts LJ, Morrow JD. Analgesic-antipyretic and antiinflammatory agents and drugs employed in the treatment of gout. In: Hardman JG, Limbird LE, eds. Goodman & Gilman’s the Pharmacological Basis of Therapeutics. 10th ed. New York: McGraw-Hill; 2001: 687-731. 9. Available at: http://www.answers.com/ nsaids. Accessed May 9, 2006. 10. Ulrich CM, Bigler J, Potter JD. Non-steroidal anti-inflammatory drugs for cancer prevention: promise, perils and pharmacogenetics. Nat Rev Cancer. 2006 Feb;6(2):130-40. 11. Itzkowitz SH, Yio X. Inflammation and cancer IV. Colorectal cancer in inflammatory bowel disease: the role of inflammation. Am J Physiol Gastrointest Liver Physiol. 2004 Jul;287(1):G7-17. 12. Wang D, Dubois RN. Prostaglandins and cancer. Gut. 2006 Jan;55(1):115-22. 13. Bruce DF. Nutritional strategies for conquering colon cancer. Life Extension. March, 2005:48-56. 14. Available at: http://www.abc.net.au/worldtoday/content/2005/s1499391.htm. Accessed April 27, 2006. 15. Available at: http://www.emaxhealth.com/ 101/3662.html. Accessed April 27, 2006. 16. Rahme E, Ghosn J, Dasgupta K, Rajan R, Hudson M. Association between frequent use of nonsteroidal anti-inflammatory drugs and breast cancer. BMC Cancer. 2005 Dec 12;5:159. 17. Schildkraut JM, Moorman PG, Halabi S, Calingaert B, Marks JR, Berchuck A. Analgesic drug use and risk of ovarian cancer. Epidemiology. 2006 Jan;17(1):104-7. 18. Baron JA, Cole BF, Sandler RS, et al. A randomized trial of aspirin to prevent colorectal adenomas. N Engl J Med. 2003 Mar 6;348(10):891-9. 19. Sandler RS, Halabi S, Baron JA, et al. A randomized trial of aspirin to prevent colorectal adenomas in patients with previous colorectal cancer. N Engl J Med. 2003 Mar 6;348(10):883-90. 20. van de Pol LA, Hensel A, Barkhof F, Gertz HJ, Scheltens P, van der Flier WM. Hippocampal atrophy in Alzheimer disease: age matters. Neurology. 2006 Jan 24;66(2):236-8. 21. Available at: http://www.nia.nih.gov/ Alzheimers/ResearchInformation/NewsReleases/Archives/PR1997/PR19970310NSAID.htm. Accessed April 27, 2006. 22. Ho L, Pieroni C, Winger D, et al. Regional distribution of cyclooxygenase-2 in the hippocampal formation in Alzheimer’s disease. J Neurosci Res. 1999 Aug 1;57(3):295-303. 23. Roman GC. Vascular dementia: distinguishing characteristics, treatment, and prevention. J Am Geriatr Soc. 2003 May;51(5 Suppl Dementia):S296-S304. 24. Zandi PP, Anthony JC, Hayden KM, et al. Reduced incidence of AD with NSAID but not H2 receptor antagonists: the Cache County Study. Neurology. 2002 Sep 24;59(6):880-6. 25. in ‘t, V, Launer LJ, Breteler MM, Hofman A, Stricker BH. Pharmacologic agents associated with a preventive effect on Alzheimer’s disease: a review of the epidemiologic evidence. Epidemiol Rev. 2002;24(2):248-68. 26. Etminan M, Gill S, Samii A. Effect of non-steroidal anti-inflammatory drugs on risk of Alzheimer’s disease: systematic review and meta-analysis of observational studies. BMJ. 2003 Jul 19;327(7407):128. 27. Nilsson SE, Johansson B, Takkinen S, et al. Does aspirin protect against Alzheimer’s dementia? A study in a Swedish population-based sample aged > or =80 years. Eur J Clin Pharmacol. 2003 Aug;59(4):313-9. 28. Husain S, Andrews NP, Mulcahy D, Panza JA, Quyyumi AA. Aspirin improves endothelial dysfunction in atherosclerosis. Circulation. 1998 Mar 3;97(8):716-20. 29. Available at: http://www.cnn.com/HEALTH/ library/DS/00691.html. Accessed May 8, 2006. 30. Steinhubl SR, Moliterno DJ. The role of the platelet in the pathogenesis of athero-thrombosis. Am J Cardiovasc Drugs. 2005;5(6):399-408. 31. Libby P, Ridker PM, Maseri A. Inflammation and atherosclerosis. Circulation. 2002 Mar 5;105(9):1135-43. 32. Eidelman RS, Hebert PR, Weisman SM, Hennekens CH. An update on aspirin in the primary prevention of cardiovascular disease. Arch Intern Med. 2003 Sep 22;163(17):2006-10. 33. Available at: http://foxnews.webmd.com/ content/article/115/111752.htm. Accessed April 27, 2006. 34. Berger JS, Roncaglioni MC, Avanzini F, Pangrazzi I, Tognoni G, Brown DL. Aspirin for the primary prevention of cardiovascular events in women and men: a sex-specific meta-analysis of randomized controlled trials. JAMA. 2006 Jan 18;295(3):306-13. 35. Hayden M, Pignone M, Phillips C, Mulrow C. Aspirin for the primary prevention of cardiovascular events: a summary of the evidence for the US Preventive Services Task Force. Ann Intern Med. 2002 Jan 15;136(2):161-72. 36. Available at: http://www.americanheart.org presenter.jhtml?identifier=4704. Accessed April 26, 2006. 37. Savon JJ, Allen ML, DiMarino AJ Jr, Hermann GA, Krum RP. Gastrointestinal blood loss with low dose (325 mg) plain and enteric-coated aspirin administration. Am J Gastroenterol. 1995 Apr;90(4):581-5. 38. Bowman J. Strokes. Upper Saddle River, NJ: Prentice Hall; 2003. 39. Anon. Aspirin for the primary prevention of cardiovascular events: recommendation and rationale. Ann Intern Med. 2002 Jan 15;136(2):157-60. 40. Ridker PM, Cook NR, Lee IM, et al. A randomized trial of low-dose aspirin in the primary prevention of cardiovascular disease in women. N Engl J Med. 2005 Mar 31;352(13):1293-304. 41. Grundy SM. Metabolic syndrome: therapeutic considerations. Handb Exp Pharmacol. 2005;(170):107-33. 42. Dempster DW, Rosenstock JL, Scwimmer JA, Panagopoulos G, DeVita MV, Michelis MF. Underutilization of aspirin in hemodialysis patients for primary and secondary prevention of cardiovascular disease. Clin Nephrol. 2005 Nov;64(5):371-7. 43. Hankey GJ, Norman PE, Eikelboom JW. Medical treatment of peripheral arterial disease. JAMA. 2006 Feb 1;295(5):547-53. 44. Kelemen MD. Angina pectoris: evaluation in the office. Med Clin North Am. 2006 May;90(3):391-416. |


{kind=link}
Wellness
Specialists
1-800-226-2370 - This service is FREE
7:30 AM - 12 AM (ET) Mon-Fri | 9 AM - 12 AM (ET) Sat-Sun