
Tinnitus
Tinnitus
Last Section Update: 08/2023
Contributor(s): Maureen Williams, ND; Shayna Sandhaus, PhD; Stephen Tapanes, PhD; Franco Melis
1 What is Tinnitus?

Tinnitus is the perception of sound for which there is no identifiable corresponding sound source.1,2 It is often described as “ringing” in the ears, but does not necessarily involve a ringing sound. Tinnitus may be perceived as buzzing, hissing, grinding, or other similar sounds.3 While not a disease itself, chronic tinnitus is almost always a symptom of an underlying condition.4
An estimated 10–30% of adults have tinnitus, and the prevalence increases with age.2,5,6 In addition to older age, tinnitus is more likely in those with hearing loss, a history of loud noise exposure, and head or neck trauma.5,7,8
Although many people with tinnitus are not bothered by it, some tinnitus sufferers experience co-occurring symptoms such as anxiety, depression, insomnia, diminished hearing, or increased hearing sensitivity that diminish their quality of life.2 While emotional distress may be directly related to the perception of chronic noise in the ears,9 tinnitus may also interfere with normal sleep patterns, which could eventually contribute to cognitive and emotional problems.10
Although chronic tinnitus is not curable, several treatment strategies can help improve quality of life for people with tinnitus. The approach to treatment depends on the individual but may include cognitive behavioral therapy, hearing aids, various types of sound therapy, neuronal modulation, medication, or cochlear implants. In addition, nutritional supplements like ginkgo, melatonin, coenzyme Q10, zinc, and vitamin B12 have all shown positive effects as part of tinnitus treatment.
2 The Experience of Tinnitus
People with tinnitus perceive sound in one or both ears or in the head, despite the lack of an identifiable sound source. Various words can describe the phenomenon of tinnitus, including ringing, buzzing, whistling, hissing, rushing, crackling, beeping, or simply an unpleasant sound. The sound may be simple, as in a single tone, or complex, including multiple tones, and can change markedly from moment to moment. Although as many as 30% of individuals are estimated to experience tinnitus, only about 5% of adults report having troublesome tinnitus that negatively impacts their day-to-day life.11
The experience of tinnitus can vary substantially between people and with underlying cause; therefore, tinnitus is generally described and categorized according to its characteristics (Table 1). Most cases of tinnitus are subjective, chronic, non-pulsatile, tonal, and bilateral.
| Table 1: Tinnitus Subtypes and Characteristics2,12-14 | |
|---|---|
| Type, by opposing characteristics | Description |
| Primary vs. Secondary |
Tinnitus with no readily identifiable cause aside from age-related hearing loss or noise-induced hearing loss is said to be “primary” tinnitus. Primary tinnitus is the more common type. Tinnitus that can be attributed to an underlying cause other than hearing loss (age-related or noise-induced) is called “secondary” tinnitus. For instance, secondary tinnitus might be due to an infection, metabolic or neurological disease, head or neck injury, or medication use. |
| Subjective vs. Objective |
Subjective tinnitus is strictly phantom sound perception. This is the main focus of this Protocol. Objective tinnitus is actual noise produced inside the body by anatomic or physiologic phenomena and can be heard by an outsider. |
| Peripheral vs. Central |
Peripheral tinnitus is caused by dysfunction of the peripheral auditory system (ie, the cochlea of the inner ear). Central tinnitus is caused by dysfunction in the central auditory system of the brain. |
| Chronic vs. Acute |
Tinnitus lasting for three months or longer is generally considered chronic. This Protocol is focused on chronic tinnitus. Acute tinnitus usually refers to tinnitus that resolves on its own in less than three months. |
| Non-pulsatile vs. Pulsatile |
In most cases of hearing loss or noise-induced tinnitus, the perceived sound is non-pulsatile (not pulsating), but some neurologic disorders can also cause non-pulsatile tinnitus. This Protocol is mainly about non-pulsatile tinnitus. The perception of a pulsating sound (often described as rhythmic “thumping” or “whooshing”) can be an indicator of an underlying vascular problem, such as intracranial hypertension, systemic hypertension, or a vascular malformation or tumor. It can also be due to muscular contractions in or around the ears. |
| Tonal vs. Non-tonal |
Tonal tinnitus, which is the more common type, involves tonal sounds such as ringing, whistling, or buzzing. Non-tonal tinnitus involves non-tonal sounds such as crackling, clicking, or rumbling. |
| Constant vs. Intermittent |
Constant tinnitus never abates. Intermittent tinnitus includes periods without symptoms. |
| Bilateral vs. Unilateral |
Bilateral tinnitus is experienced on both sides. Unilateral tinnitus is experienced on one side only. Because unilateral tinnitus can be a symptom of stroke, tumor, or neurological disease, these possible causes should be investigated. |
Subjective data collected from tinnitus sufferers indicates tinnitus loudness and related distress are increased during the nighttime and early morning hours.15 Tinnitus loudness has been closely correlated with tinnitus distress. Furthermore, the relationship between tinnitus loudness and the distress it causes appears to be stronger in the context of intense emotions, negative emotions, and high stress levels.16,17
In a study of 49 patients seeking care for tinnitus with a duration of less than 28 days, only nine (18.4%) became tinnitus-free within three to six months.18 Little is known about the progression of chronic tinnitus over time, but evidence suggests most tinnitus sufferers experience some gradual improvement.18,19 In chronic tinnitus sufferers for whom this type of improvement or habituation does not occur, it is thought anxiety triggered by tinnitus causes reinforcement of tinnitus perception, leading to more anxiety in a vicious cycle of distress and tinnitus.2
A meta-analysis that examined long-term outcomes in subjects assigned to “no intervention” or “waiting list” groups in controlled trials for tinnitus treatments showed self-reported measures of tinnitus improved over time. Tinnitus has been reported to resolve completely after years or even decades of persistence in some cases, but this appears to be rare.19
In an observational study that included 388 patients seen in a chronic tinnitus clinic (most of whom had tried at least one type of tinnitus treatment), a follow-up survey administered about one to six years later showed tinnitus distress had generally diminished. Improvements were seen in patient ratings of tinnitus severity, annoyance, unpleasantness, and discomfort; however, the characteristics of the tinnitus, presence of depression, and ratings of quality of life and overall health were unchanged.20 In another study, 300 patients who had received various individualized treatments (eg, hearing aids and internal or external sound generators) at a tinnitus clinic answered a questionnaire at their first clinic visit and again between six and 36 months later. The results indicated overall reductions in tinnitus loudness and severity, as well as tinnitus-related anxiety and the presence of depression. Patients whose sleep improved had greater reductions in tinnitus severity compared with those who continued to suffer from insomnia.21 On the other hand, a study that followed 4,746 individuals with tinnitus for four years found 18.3% of cases resolved, 9% improved, 9% worsened, and about 64% experienced no change,22 and a study in which a questionnaire was administered to 528 tinnitus patients found 25% reported the severity of their tinnitus had increased since its onset.23
3 What are the Main Risk Factors for Tinnitus?
Tinnitus is a symptom that has been associated with a number of factors and conditions. The most strongly correlated risk factors include4,24:
- Hearing loss. Hearing loss is a well-established risk factor for tinnitus.7,24 Approximately 68% of individuals with tinnitus have some degree of hearing loss; in addition, tinnitus has been reported to be a symptom in 48% of people with hearing loss.4,7 The link between hearing loss and tinnitus has been suggested to be due to a compensatory effect: the brain compensates for decreased activation of the auditory nerve (which carries signals from the cochlea to the brain) by increasing “gain” or signal amplification in the auditory system of the brain, as well as decreasing auditory signal inhibition, which may result in tinnitus and possibly hypersensitivity to noise.2,25 Individuals with tinnitus should undergo a hearing test.
- Older age. Older individuals have an increased risk of tinnitus.26 This may be due in part to age-related changes in cochlear structures and nerve function and connectivity.26,27 Older people are also more likely to experience tinnitus-related distress.28
- Chronic and/or high-intensity noise exposure. Long-term exposure to loud noise, whether at work or during leisure activities (eg, listening to loud music, live or through headphones), is well known to increase the chance of developing tinnitus, but evidence also shows even a single exposure to extremely loud noise, such as during military combat, can cause chronic tinnitus.24 In fact, tinnitus is one of the most common disabilities among veterans.29 Workers in music and construction industries have also been found to have higher rates of tinnitus than those in quieter fields.30
- Physical trauma. Ear, head, and neck trauma are frequently associated with tinnitus. As many as 53% of individuals who have experienced traumatic brain injury develop tinnitus.8
- Smoking. A history of smoking has been shown to increase the risk of developing tinnitus.31
- History of ear infections. Chronic ear infection (otitis media) in childhood has been linked to increased risk of tinnitus in adulthood.32
4 How is Tinnitus Diagnosed?
Because tinnitus is a perception disorder, there is currently no objective test to diagnose the condition. However, there are various tests and protocols audiologists can use to help evaluate and diagnose tinnitus.71 Questionnaires may be used to assess the effects and burden of tinnitus on daily life.71,72
The diagnostic workup for tinnitus begins with a comprehensive medical history evaluation. This will include a medication review and physical exam to identify treatable causes of tinnitus or danger signs in the nature of the tinnitus, such as if it is sudden onset, pulsatile, unilateral or asymmetric, or accompanied by hearing loss or other neurological changes. If danger signs are observed, immediate evaluation may be needed. Imaging tests may be ordered in cases with red flag signs; however, in patients with non-pulsatile bilateral tinnitus, with or without symmetric hearing loss, and an otherwise normal history and physical exam, imaging is not necessary.12
A comprehensive audiological exam may be appropriate in patients with tinnitus lasting six months or longer, those with one-sided tinnitus, accompanying hearing changes, and tinnitus-related distress.12 During audiological testing, the patient generally listens for and indicates when they hear tones of various frequencies and intensities, which may be transmitted through the air or through headphones. Such testing assesses the function of the middle and inner ear structures and can help detect and quantify hearing loss. It can also be used to identify tinnitus pitch, loudness, and other qualities that could help guide therapy.71,72
5 What Causes Tinnitus?
The cause of primary tinnitus is not known, but is thought to be multifactorial, involving multiple physiologic and possibly genetic mechanisms.4 Dysfunction of the cochlea (the inner ear structure responsible for turning vibrations into nerve signals), abnormal nerve signaling in the brain auditory system, or a combination of the two play a key role in tinnitus onset and persistence.4,74 In addition, networks that connect the auditory system with other brain regions may become involved. For example, activation of the limbic and paralimbic systems, which are responsible for behavioral and emotional responses, are thought to contribute to distress signaling and complications of tinnitus, such as cognitive, mood, and sleep disorders, in some individuals.2,75,76
Damage to hair cells in the cochlea has been suggested to trigger the onset of tinnitus in many cases. Hair cells detect movement in the environment and transform it into auditory and vestibular nerve signals, and can be damaged by factors such as aging, noise trauma, and toxicity.26,74 It is thought damaged hair cells release excessive amounts of glutamate, the main excitatory neurotransmitter, causing dysfunctional nerve activation that can result in tinnitus.26 Simultaneous increased activation of multiple auditory system nerve fibers is believed to be an important mechanisms underlying tinnitus. Loss of nerve transmission inhibition, leading to increased excitability of nerve fibers involved in auditory perception, may also play a role. Another possible contributing mechanism is maladaptive neuroplasticity, in which neuronal pathways adapt and conform pathologically to changes in auditory system nerve signaling.75
In secondary tinnitus, a known cause exists. Examples of causes of secondary tinnitus include12:
- Vascular conditions that generate an internal perceivable sound
- Musculoskeletal causes, such as head or neck injury or temporomandibular joint dysfunction
- Use of ototoxic medications
- Bacterial, viral, or fungal infections
- Trauma to the auditory structure, such as the ear drum
- Earwax impaction or improper earwax cleaning procedures77,78
- Metabolic disturbance, such as diabetes or imbalanced lipid levels
- Neurological conditions, such as intracranial hypertension or vestibular migraine
- Other problems affecting the outer and middle ear, such as cerumen impaction, tumors, fusing of the middle ear bones, or dysfunction of the tympanic membrane or eustachian tubes
Medications that Can Cause Tinnitus
Many medications are known to have toxic effects on auditory tissues and can cause or worsen tinnitus (Table 2), especially when used long-term and/or at high doses. For most of these medications, tinnitus is an uncommon or rare potential side effect; nevertheless, if you experience tinnitus and are taking any of these medications, check with your doctor to see if your medications may be contributing to your tinnitus.12,79
| Table 2: Medications that Can Cause Tinnitus | |
|---|---|
| Medications | Examples |
| Non-steroidal anti-inflammatory drugs (NSAIDs) and analgesics80,81 |
|
| Some blood pressure-lowering drugs60,81 |
|
| Phosphodiesterase type 5 inhibitors12 |
|
| Some antibiotics81 |
|
| Some antiviral drugs12 |
|
| Antimalarial drugs12,79,82 |
|
| Some antiseizure drugs12 |
|
| Immune suppressants12 |
|
| Some anticancer drugs12,79,81 |
|
| Oral contraceptives83 |
|
| Miscellaneous drugs12 |
|
Headphone Use and Tinnitus
Listening to music through personal listening devices paired with headphones or earphones is increasingly common, but studies have shown listening to music through headphones can easily expose the listener to noise trauma-inducing sound levels.84 Frequent exposure to loud music, including through headphones, can cause auditory system damage that may lead to tinnitus and hearing loss.85
A systematic review found more than 58% of adolescents and young adults participating in 26 studies exceeded safe daily noise exposures by listening to loud music through headphones, and this habit was correlated with signs of damage to the auditory system.86
According to the U.S. National Institute for Occupational Safety and Health, there are two easily detectible signs that music–or any noise–levels are unsafe87:
- If you have to raise your voice to talk to someone who is an arm’s length away because of the music or noise
- If your ears are ringing or sounds seem dull or flat after the music or noise stops
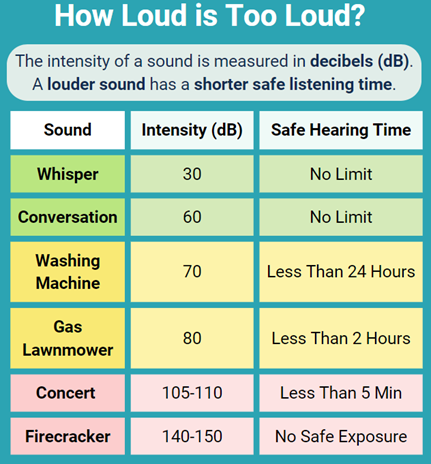
In general, sounds that are at or below 70 A-weighted decibels (dBA, the unit used to describe loudness specifically for humans) are considered safe, while sounds at or above 85 dBA are more likely to cause damage over time. For context, gas-powered leaf blowers, lawn mowers, and city traffic (from inside a car) generate a noise level of 80–85 dB. Alarmingly, many headphones/earbuds/speakers can reach 94–110 dBA at their maximum volume. Fortunately, most modern phones and other listening devices have settings that allow the user to limit the maximum decibel output of their device.
6 Nutrients

Ginkgo
Ginkgo (Ginkgo biloba) leaves are widely used to enhance peripheral and cerebral blood flow and support brain health. Preclinical evidence suggests ginkgo has positive effects on tinnitus.88 For example, a study using an animal model of noise trauma-induced hearing loss and tinnitus found treatment with ginkgo restored hearing, reduced tinnitus-related behaviors, and normalized brain signaling.89
In a randomized controlled trial, 33 participants with tinnitus and hearing loss were treated for 90 days with 240 mg of ginkgo extract, hearing aids, or both; all three treatments led to reduced tinnitus loudness and severity after 90 days, and ginkgo was effective regardless of tinnitus duration.90 In another controlled trial, 86 tinnitus patients received either a single intratympanic injection of caroverine (Tinnitin) (a glutamate-blocking muscle-relaxing drug used in Austria and Switzerland to treat tinnitus), oral ginkgo extract for three months, a placebo injection, or oral placebo for three months. The dosage of gingko used in this study was 60 mg twice daily. Both ginkgo and caroverine were more effective than placebo. The initial response rate to caroverine was a bit better than that to ginkgo, but the response rates converged by six months. The authors concluded that, for severe tinnitus, an initial treatment with caroverine is warranted, followed by twice daily ginkgo for three months to provide lasting relief.91 In a three-month trial, 90 subjects with tinnitus were treated with ginkgo extract (60 mg twice daily), betahistine (Serc), or trimetazidine (Vastarel) (a drug that dilates coronary and other peripheral blood vessels, but is not available in the United States); all three treatments led to significant reductions in tinnitus severity, but ginkgo had the smallest effect.92
Despite a number of clinical trials finding ginkgo had positive effects on tinnitus, some clinical trials have found no benefit.93 A meta-analysis published in 2004 of findings from randomized placebo-controlled trials found 21.6% of subjects with tinnitus who were given ginkgo improved, while 18.4% of those given placebo improved, a difference that was not statistically significant.94 More recent reviews of the contradictory findings have concluded that ginkgo is not likely to be consistently beneficial as a treatment for tinnitus, although certain individuals may experience improvement.93,95
Individuals with tinnitus who also have dementia may be particularly likely to benefit from treatment with ginkgo. One analysis used pooled data from five randomized placebo-controlled trials in which ginkgo, at 240 mg daily for 22–26 weeks, was tested as a therapy for dementia; the analysis found, in a subset of 773 participants with tinnitus, ginkgo was more effective than placebo for reducing tinnitus severity.96 A similar study examined data from three randomized placebo-controlled trials investigating the effects of ginkgo extract, at a dose of 240 mg daily for 22–24 weeks, in subjects with mild-to-moderate dementia along with anxiety or depression; this study found, in the 594 participants who had tinnitus, ginkgo extract reduced tinnitus severity, reduced anxiety and depression, and improved cognition. After analyzing the data, the study authors estimated 60% of ginkgo’s effect on tinnitus was due to direct effects while the remaining 40% of its effect was related to improved mood and cognitive function.97
Melatonin
Melatonin is a hormone that regulates circadian cycles and scavenges free radicals.98 Melatonin is thought to reduce tinnitus by protecting hair cells (sensory cells in the ear responsible for hearing) from oxidative damage, promoting normal blood flow to inner ear structures, relaxing ear muscles, attenuating depression and anxiety, inhibiting the stress response, and supporting normal sleep patterns.99,100 Preclinical evidence suggests melatonin protects ear tissues against the ototoxic (toxic to the ear) effects of certain medications.101 In an observational study that included 139 elderly subjects, blood melatonin levels were lower in those with tinnitus than those without tinnitus.102
A review of the clinical evidence found melatonin therapy can improve sleep in individuals with tinnitus, but was unable to determine conclusively whether it can improve tinnitus.103 In one randomized clinical trial in 70 volunteers with chronic tinnitus, both 3 mg of melatonin daily and a standard dose of sertraline (Zoloft) (an antidepressant medication) for three months reduced tinnitus severity, but melatonin was more effective.104 Another randomized controlled trial in 60 subjects with acute tinnitus (of three months or shorter duration) found intratympanic dexamethasone enhanced the effectiveness of melatonin after three months of therapy.105
A combination of melatonin and sulodexide has been tested as a therapy for tinnitus. Sulodexide is a naturally occurring compound composed of heparin sulfate and dermatan sulfate. It is derived from the intestinal mucosa of pigs and is used in some parts of the world to prevent venous blood clots and treat chronic disorders of the veins.106 In an uncontrolled trial that included 30 tinnitus patients treated with 3 mg of melatonin nightly plus sulodexide twice daily, tinnitus improved in 90% of participants after 80 days of treatment.107 A randomized controlled trial included 102 tinnitus patients who received either melatonin (3 mg nightly) plus sulodexide, melatonin (3 mg nightly) alone, or no treatment for 80 days. Both treatment regimens resulted in tinnitus improvement compared with no treatment, but melatonin plus sulodexide was found to be more effective than melatonin alone.108
Coenzyme Q10
Coenzyme Q10 (CoQ10), an antioxidant enzyme needed for cellular energy production, has demonstrated anti-inflammatory, neuro-protective, cardio-protective, and other health-promoting properties.109 An observational study that included 200 participants with tinnitus found 38.5% had decreased blood levels of CoQ10.70 In addition, a clinical trial in 20 individuals with tinnitus found supplementing with CoQ10 (300 mg per day of ubiquinone formulated with ethyl alcohol and lecithin) for 12 weeks led to reductions in scores on a tinnitus questionnaire in a subset of participants whose blood CoQ10 levels were low at the beginning of the trial.110
Supplementing with CoQ10 has been shown to protect hair cells from noise trauma in animals and shorten the time needed for hearing recovery after experimental exposure to loud noise in humans.111,112 Taking a water-soluble CoQ10 (160 mg) plus other nutrients (B vitamins, vitamin E [36 mg], choline [100 mg], melatonin [1 mg], ginkgo phytosome [80 mg], and milk protein hydrolysate [150 mg]) appeared to protect against hearing damage and tinnitus in a pilot trial that included 26 cancer patients being treated with cisplatin (Platinol), a chemotherapy agent known to have ototoxicity.113 This same combination, but with 5 mg of melatonin, was given to 30 individuals in a separate clinical trial and was found to reduce duration of noise-induced tinnitus and shorten the time to hearing recovery after a 10-minute exposure to loud noise. The participants in this trial took the formulation once daily for 30 days and the second test occurred after the 30-day supplementation period.112
Zinc
Zinc is a micronutrient involved in numerous biological processes and found throughout the body.114 Among other things, it is necessary for normal immune function, control of oxidative stress, and modulation of the responsiveness of brain neurons.114,115
A study with 200 participants with tinnitus found zinc levels were low in 30.6% of the men in the study but not in the women.70 Another study that included 100 tinnitus patients found zinc levels declined with aging and low levels were associated with increased tinnitus loudness and severity.116 Nevertheless, several large observational studies have found, overall, that blood zinc levels were not significantly decreased in tinnitus sufferers.117,118
Clinical trials investigating zinc’s effects on tinnitus have yielded mixed results. An uncontrolled preliminary trial examined the effect of zinc on tinnitus and hearing in 20 individuals with noise-induced hearing loss and chronic tinnitus, 18 (90%) of whom continued to be exposed to loud noise in their work environment during the trial. After supplementing with 156 mg zinc gluconate (providing 20 mg of elemental zinc) twice daily for two months, scores on a standardized assessment of the impact of tinnitus on quality of life were found to have improved significantly in 17 (85%) of participants; however, zinc therapy had no effect on tinnitus loudness or intensity and did not improve hearing.119 Similarly, a randomized controlled trial in 41 tinnitus patients found 50 mg of zinc daily for two months resulted in reduced subjective assessment of tinnitus severity in 82% of those receiving zinc, but there was not a statistically significant reduction in tinnitus loudness.120 Several other trials have found zinc did not have a significant effect on tinnitus.121-123
Vitamin B12 and Other B-Complex Vitamins
Vitamin B12 is needed for healthy function of nerves and blood vessels, and B12 deficiency can cause nerve damage resulting in a range of neurological symptoms, including tinnitus.124 Low vitamin B12 levels and intake have been associated with increased risk of tinnitus in observational studies.102,125 In a study that included 113 military personnel exposed to loud noise, B12 deficiency was detected in 47% of those with tinnitus plus noise-induced hearing loss, 27% of those with noise-induced hearing loss only, and 19% of those with normal hearing, suggesting B12 deficiency may be associated with risk of developing tinnitus.126
In a randomized controlled trial, 40 patients with tinnitus (17 of whom also had vitamin B12 deficiency with levels below 250 pg/mL) were treated with weekly intramuscular injections providing 2,500 mcg vitamin B12 or saline (placebo) for six weeks. Vitamin B12 injections were found to improve tinnitus in those with B12 deficiency.127 Another clinical trial in 50 patients with tinnitus, half of whom also had hearing loss, found treatment with intramuscular injections providing 100 mg vitamin B1, 100 mg vitamin B6, and 1,000 mcg vitamin B12 twice weekly led to tinnitus improvement mainly in those without hearing loss.128 However, another small uncontrolled trial found that B12 replacement therapy did not improve tinnitus regardless of baseline B12 status.129
Korean Red Ginseng
Korean red ginseng (Panax ginseng, also known as Chinese or Asian ginseng) has been used in traditional herbal medicine throughout Asia to treat a broad range of health conditions including fatigue, stress, and age-related ailments. Extracts from ginseng have demonstrated immune-modulating, anti-inflammatory, oxidative stress-reducing, antimicrobial, and anticancer properties, as well as the ability to improve metabolism and counter the debilitating effects of stress.130 In an open controlled clinical trial, 61 subjects with chronic tinnitus received either 1,500 mg or 3,000 mg of Korean red ginseng daily, or 160 mg of ginkgo extract (as a control), for four weeks. Scores on the Tinnitus Handicap Inventory improved only in the group receiving 3,000 mg of Korean red ginseng, but measures of tinnitus loudness and intensity and health-related quality of life did not improve significantly in any group.131
Pycnogenol
Pycnogenol is a compound extracted from French maritime pine bark and known to have free radical scavenging and anti-inflammatory effects. One randomized controlled trial compared the effects of Pycnogenol to no treatment in 92 individuals with mild-to-moderate, sudden-onset, one-sided tinnitus of unknown origin lasting at least two weeks. After four weeks, those treated with Pycnogenol, at dosages of either 150 mg or 100 mg daily, had increased cochlear blood flow in the affected ear and reduced tinnitus severity, and the effects were more pronounced in those receiving the higher dosage.132 Another controlled trial that included 120 subjects with tinnitus and low cochlear blood flow related to Ménière disease found 150 mg of Pycnogenol per day for six months improved cochlear blood flow and reduced subjective measures of tinnitus compared with no treatment; in addition, 87.3% of subjects taking Pycnogenol were free of Ménière disease symptoms after six months.133
Magnesium
Magnesium is an electrolyte nutrient important for many aspects of healthy cellular function. In nerves, magnesium protects against damage due to excessive excitation134; in blood vessels, magnesium reduces blood vessel calcification and promotes healthy blood flow by relaxing smooth muscles in blood vessel walls.135,136 An observational study that included 76 tinnitus sufferers and 86 healthy controls found blood magnesium levels were lower in those with tinnitus.137 In a preliminary uncontrolled trial, 26 participants with tinnitus were found to have reduced tinnitus severity after treatment with 532 mg of magnesium per day for three months.138
Vitamin D
Vitamin D plays an important role in regulating calcium metabolism and immune function, and adequate levels are important for cardiovascular, metabolic, and neurological health. In fact, low vitamin D levels have been linked to the onset and progression of neurological disorders such as migraine headache, diabetic neuropathy, multiple sclerosis, Alzheimer disease, and Parkinson disease.139 An observational study that included 201 individuals with tinnitus and 99 with no tinnitus found vitamin D deficiency (<20 ng/mL) was more than twice as common in tinnitus sufferers: 50.7% of those with tinnitus versus 22.2% of those without tinnitus had vitamin D deficiency. In addition, increased tinnitus severity and loudness were correlated with severely decreased (≤15 ng/mL) blood vitamin D levels.140 A meta-analysis published in 2023 analyzing three observational studies identified that serum vitamin D levels were 22% lower in patients with tinnitus compared to those without, suggesting lower vitamin D levels may be a contributing factor to tinnitus.141
Acai
Acai berries are known for their rich flavonoid content and strong antioxidant and anti-inflammatory effects. In a randomized placebo-controlled trial that included 30 individuals with tinnitus and no-to-mild hearing loss, 100 mg acai extract daily for three months reduced self-reported tinnitus-related discomfort, but did not lower anxiety levels or improve markers of oxidative stress more than placebo.142
Taurine
Taurine is a non-essential amino acid that is mainly obtained in the diet but can also be made in the liver and kidney from the amino acids cysteine and methionine.143,144 Taurine has anti-inflammatory and oxidative stress-reducing effects, and has been shown to protect nerve tissue against oxidative and toxic injury, reduce glutamate-induced hyperactivation of nerves, and promote inhibitory nerve signaling.143-145 In an observational study, lower taurine levels were correlated with the presence of tinnitus.146 Preclinical research has shown taurine can reduce damage to hair cells and stimulate regeneration of the auditory nerve.147,148 In animal research, noise trauma was found to lower brain taurine levels,149 and taurine supplementation decreased noise-induced nerve activation.150
Other Antioxidants & Multi-nutrient Formulas
Oxidative damage to hair cells and other auditory tissues is thought to be an important contributing mechanism in tinnitus, and many therapies shown to be beneficial have antioxidant properties.151 Observational evidence suggests people with tinnitus have higher levels of markers of oxidative stress than those without tinnitus.152,153 In an animal study, the polyphenol resveratrol protected against toxin-induced tinnitus.154
Some clinical research also indicates a positive role for antioxidant supplements in tinnitus treatment. In one randomized placebo-controlled trial that enrolled 70 participants with tinnitus, 300 mg lipoic acid twice daily plus a multi-nutrient antioxidant tablet once daily for three months resulted in reduced tinnitus discomfort, loudness, and intensity.155 The multi-nutrient tablet provided:
|
|
In an uncontrolled clinical trial that included 31 participants with one-sided tinnitus, 18 weeks of treatment with a multi-nutrient supplement, providing glycerophosphorylcholine (55 mg/day), glycerophosphorylethanolamine (45 mg/day), beta-carotene (6,000 mcg RAE/day), vitamin C (180 mg/day), and vitamin E (10 mg/day), led to reductions in tinnitus loudness and discomfort.156 On the other hand, another randomized controlled trial compared the effects of three different treatment approaches (120 mg ginkgo/day, 60 mg alpha-lipoic acid plus 600 mg vitamin C/day, and 100 mg papaverine hydrochloride [Pavacot, a vasodilating drug that increases brain blood flow] plus 400 mg vitamin E) to placebo in 58 tinnitus patients aged 60 years and older. After six months, there were no significant changes in tinnitus severity in any of the treatment groups.157 In a prospective interventional study that enrolled 61 patients given a commercial combination containing 5-hydroxytryptophan, Ginkgo biloba, magnesium, melatonin, vitamin B5 and B6, and zinc twice daily, tinnitus loudness was significantly decreased after three months of treatment.158
7 How is Tinnitus Treated?

Tinnitus has many possible causes and manifestations, and no single treatment approach is effective in every case. Therapies targeting associated conditions can sometimes reduce tinnitus’ negative impacts.4
Non-invasive therapies that aim to mask or reduce perception of the bothersome sound may further reduce or relieve persistent tinnitus. In severe cases that do not respond to first-line approaches, external therapies that modulate nerve function and more invasive treatments such as medications, deep brain stimulation, and cochlear implants may be considered.4,75
Cognitive Behavioral Therapy
Cognitive behavioral therapy (CBT) is a form of psychotherapy that helps individuals incorporate conscious thought patterns and behaviors that reduce suffering and support health. CBT may be useful for improving sleep, depressive symptoms, emotional tension, and worry, which may reduce tinnitus, as well as increase effectiveness of other tinnitus therapies.159,160 In fact, of all tinnitus therapies, CBT has the strongest body of evidence showing benefits.161
A comprehensive review that included 28 studies with a combined total of 2,733 participants experiencing tinnitus for at least three months found CBT may reduce the negative effect of tinnitus on quality of life.162
Hearing Aids
Hearing aids can be beneficial in tinnitus patients with or without hearing loss. Hearing aids increase the volume of ambient noise, which may be helpful in masking tinnitus.75 In addition, improved hearing by hearing aids may help reverse or normalize maladaptive brain activity in tinnitus sufferers, as well as reduce stress and anxiety by improving communication.4 Numerous studies have found hearing aids have a positive effect on tinnitus perception in those with hearing loss.163 In addition, in a clinical trial that included 91 chronic tinnitus patients without hearing loss, approximately 90% reported reductions in tinnitus loudness and annoyance after wearing hearing aids for three months to one year.164
Sound Therapy
Sound therapy involves the use of a generated sound to provide a distraction and lower the intensity of tinnitus perception. It has also been proposed to help by lowering stress and reversing maladaptive changes in brain neuronal networks involved in perpetuating tinnitus. Hearing aids or other devices can be used as sound generators, some of which can be programmed to produce sounds in an individualized fashion based on the pitch of the tinnitus.4 Although a number of studies suggest sound therapy may be a useful part of tinnitus treatment, the evidence so far is not conclusive.4,75
Tinnitus Retraining Therapy
Tinnitus retraining therapy combinestinnitus-specific counseling to develop the ability to view tinnitus as a neutral stimulus with sound therapy to decrease tinnitus-induced neuronal activation.165 A meta-analysis of 13 randomized controlled trials with a total of 1,345 participants found standard medical treatment plus tinnitus retraining therapy led to higher response rates after one, three, and six months, and reduced tinnitus-related disability more than medical treatment alone.166 However, many of the included studies were rated as lower-quality evidence. And a randomized controlled trial that included 151 subjects with tinnitus found no differences in outcomes after 18 months of treatment with tinnitus retraining therapy, tinnitus-specific counseling alone, or basic tinnitus care that involved providing educational information and guidance.167
Tailor-Made Notched Music Training
Tailor-made notched music training involves the use of music customized to exclude tonal frequencies within one octave above and below an individual’s tinnitus pitch (ie, the “notch”). In theory, this results in stimulation of auditory circuits that are not involved in tinnitus and inhibition of the hyperactivated neurons causing tinnitus.75 A small controlled trial with 23 participants suffering from chronic tinnitus found tailor-made notched music training reduced activity in auditory brain regions and tinnitus loudness more effectively than placebo music training (with a varying notch in frequency range) or no treatment after six months and one year.168 Another study showed tailor-made notched music training promoted normalization of brain activity that had been altered by tinnitus.169 However, in a comparison trial in 30 subjects with bothersome tinnitus, notched music training, unnotched music, and low-pitch white noise worked equally well at improving tinnitus both immediately and after two weeks.170
Neuronal Modulation
Both non-invasive and invasive techniques for modulating nerve activity have been used as treatments for tinnitus. These include4,171:
-
Repetitive transcranial magnetic stimulation (rTMS),
in which a wire coil that emits a pulsed magnetic field is placed over
the scalp above a target brain region. The magnetic field that is
generated can either excite or inhibit neuronal activity, depending on
the frequency. The effects of rTMS can result in long-term changes in
neural connections and patterns of neuronal activation.172
rTMS has been used to treat depression, pain, addiction, and a range of other neurological disorders.172 Numerous clinical trials have investigated the use of rTMS in chronic tinnitus, and although results have been mixed, there appear to be positive effects.4,173 In a meta-analysis that included data from 12 randomized controlled trials with a total of 717 participants, those treated with rTMS had significantly lower Tinnitus Handicap Inventory scores than those who received sham therapy at both one month and six months after treatment.174 One reason for inconsistent results may be the lack of a standardized protocol, including dose of pulses and duration of treatment.4,172
Adverse side effects from rTMS are rare, but can include dizziness and mild neurological, psychological, or cognitive changes that may be temporary or persistent. The most severe potential adverse effect is seizure.175 A meta-analysis of adverse side effect data from 15 controlled trials in tinnitus patients found rTMS was no more likely to cause negative side effects than sham treatment, and none of the studies reported seizure as an adverse effect.176
-
Electrical stimulation is another technique for
modulating nerve activity and promoting positive neuroplastic changes.4 Various types of electrical stimulation, including
stimulation of the head, ear, vagus nerve, and cerebral cortex, have
been tested as potential therapies for chronic tinnitus.177
Transcranial electrical stimulation (tES) is the most widely used
method and involves the application of a small direct or alternating
current to the scalp via two electrodes.4 A meta-analysis of
findings from 11 clinical trials (seven that used transcranial direct
current stimulation [tDCS], three that used transcutaneous electrical
nerve stimulation [TENS], and one that used electroacupuncture of the
ear) found electrical stimulation in general reduced Tinnitus Handicap
Inventory scores and measures of tinnitus loudness and distress.178
In another meta-analysis, pooled findings from 14 trials with a total
of 1,030 participants indicated tDCS can decrease tinnitus loudness and
distress.179 Thirteen clinical trials using TENS were
included in another meta-analysis that found 40% of tinnitus sufferers
treated with TENS experienced improvement.180
Despite these promising findings, questions remain regarding the best type, dose, and location of electrical stimulation for maximizing tinnitus relief.4 In addition, safety concerns around electrical stimulation therapy, especially with long-term use, have not been adequately addressed. Hearing loss, worsening of tinnitus, and visual changes, as well as sensations of tingling, pinpricks, and pain have all been reported in patients undergoing electrical stimulation for tinnitus.181
- Neurofeedback is an individualized treatment approach in which brain wave patterns are collected and fed back to the participant in real time through visual, auditory, or tactile signals.4,171 The participant is then instructed to alter the signals in a certain way, and is rewarded with positive feedback when they are successful.171 In this way, brain activity patterns associated with tinnitus relief are reinforced.182 Although some individuals with tinnitus appear to benefit from neurofeedback training, a significant proportion of people are unable to change their brain activity, limiting the usefulness of neurofeedback as a therapeutic approach to tinnitus.4,182
- Invasive brain stimulation involves the use of electrodes implanted in the brain to alter signaling in neuronal networks that are abnormally activated in tinnitus.171 Although research into brain stimulation is in its early stages, case reports of successful treatment using stimulation to the brain cortex or deeper brain structures indicate the potential for this method to be helpful in patients with severe tinnitus that has not responded to other therapies.171,177 Deep brain stimulation has a number of possible adverse side effects related to the surgery and the electrical stimulation itself. These include post-surgical infections, pain, and surgical complications; abnormal nerve activation leading to tingling and numbness, muscle spasms, and visual changes; and potentially serious neurological, cognitive, and mood changes such as forgetfulness, loss of balance, seizures, and depression.183,184
Medications
There are currently no medications approved by the U.S. Food and Drug Administration (FDA) for treating tinnitus.75 However, tinnitus can sometimes improve with medical treatments targeting associated conditions, such as high blood pressure, sleep disorders, or depression. A number of drugs have been reported to be helpful when used as off-label therapy in tinnitus patients.81 It is important to note that, paradoxically, some of the drugs used to treat tinnitus can also cause tinnitus, and none are currently recommended as primary therapies for tinnitus.75,81
Misoprostol. Limited evidence from a few preliminary trials suggests misoprostol (Cytotec) may be effective in some cases of tinnitus. However, more evidence is needed. Importantly, misoprostol can cause pregnancy termination or complications so must not be used unintentionally by women who are pregnant or may become pregnant.185-188
Antidepressants. Some evidence suggests antidepressant therapy may reduce tinnitus-related stress, anxiety, and depression.81 Small placebo-controlled trials have indicated amitriptyline (Elavil),189 nortriptyline (Pamelor),190 and sertraline191 may reduce tinnitus. Nevertheless, the evidence for antidepressants in tinnitus treatment is inconclusive.192
Anti-anxiety drugs. Alleviating tinnitus-related anxiety may help reduce the perception of tinnitus. A family of anti-anxiety drugs called benzodiazepines have been studied for their possible benefits in tinnitus sufferers. These drugs may work by interrupting signaling between auditory circuits and other brain regions. Findings from several clinical trials have suggested benzodiazepines such clonazepam (Klonopin) and oxazepam (Serax) may reduce tinnitus, although results are mixed.193,194
Anticonvulsants. A common neurological and psychological basis for tinnitus and pain disorders has been proposed. This has led to research evaluating whether chronic pain disorder treatments may be useful in tinnitus.160 Gabapentin (Neurontin) is an anticonvulsant sometimes used as an off-label therapy for chronic pain. Despite some promising findings, particularly in those with noise-induced tinnitus, gabapentin’s usefulness in tinnitus has not been clearly demonstrated.81,195
NMDA antagonists. Acamprosate (Campral), a drug that inhibits the action of glutamate on receptors known as N-methyl-D-aspartate (NMDA) receptors, is used to treat alcohol abuse disorder. NMDA receptors are thought to play a role in neuronal hyperexcitation, a likely mechanism of tinnitus.81 Acamprosate has been found to reduce tinnitus in three small randomized controlled trials.196-198 Neramexane, an investigational NMDA blocker, was found in a randomized placebo-controlled trial to reduce scores on the Tinnitus Handicap Inventory questionnaire, but not tinnitus loudness.199 More research is needed to establish whether or not these medications have the potential to help tinnitus sufferers.
Intratympanic steroid injections. Some evidence suggests steroids injected through the tympanic membrane (ear drum) may help tinnitus patients by reducing inflammation and enhancing blood flow. However, a meta-analysis of four randomized controlled trials was not able to show this treatment was more effective than placebo.200 Intratympanic steroid injections appear to be more likely to be beneficial in acute than chronic tinnitus.201
Cochlear Implants
Cochlear implants are devices that are surgically placed in the cochlea where they stimulate the auditory nerve, allowing some people with deafness to perceive sounds. They have been studied for their possible role in treatment of tinnitus accompanied by moderate-to-severe hearing loss, but findings have been mixed. The induction or worsening of tinnitus by cochlear implants has also been reported.4,202 A study that monitored 142 tinnitus patients who were treated for severe hearing loss with cochlear implants found 66% experienced suppression of tinnitus—with 37% experiencing complete resolution—one year after surgery.203 Another study that followed 25 subjects with one-sided tinnitus and hearing loss for one year found 22 of 25 participants (92%) experienced significant improvement in tinnitus beginning one to two months after implantation.204 Emerging evidence from a three-week trial in 22 chronic tinnitus patients without substantial hearing loss suggests a trans-tympanic device for stimulating the cochlea may help reduce tinnitus while preserving hearing, and represents a potential option for tinnitus sufferers without hearing loss.205
Acupuncture
Acupuncture is sometimes used to treat tinnitus, and appears to work by improving cochlear blood flow and neuronal activation.99 Although there are multiple clinical trials suggesting acupuncture and electroacupuncture are beneficial therapies in tinnitus, systematic reviews of the literature have led to questions regarding the quality of the evidence, and definitive conclusions have not been made.206-208 No adverse effects from treating tinnitus with acupuncture have been reported.99
8 Dietary & Lifestyle Changes for Tinnitus
Eating a healthy diet and being physically active may help protect against tinnitus. In a study that used data from 2,176 participants in the ongoing National Health and Nutrition Examination Survey (NHANES), those with higher Healthy Eating Index scores were less likely to report persistent tinnitus.209 Specifically, diets high in protein and fiber and low in sugars and starches have been linked to lower odds of tinnitus.98 In a study of 1,730 participants aged 50 years and older, those with lower intakes of fiber from fruit and cereal grains were 65% and 54%, respectively, more likely to have tinnitus than those with higher intakes.210 A study that compared the diets of 185 tinnitus patients to those of 198 matched controls without tinnitus found diets that included a wide diversity of foods, and higher consumption of high-protein foods, coffee and butter were correlated with lower risk of tinnitus.211 Another study based on data from 3,826 NHANES participants found being physically active was also associated with lower likelihood of having tinnitus.212
On the other hand, few studies have examined whether lifestyle changes after the onset of tinnitus are helpful.22 In two randomized controlled trials, one with 46 and the other 63 subjects with obesity and tinnitus, a diet and exercise weight loss intervention was found to reduce tinnitus severity and improve quality of life, particularly in participants who lost 5% or more of their body weight.66,67 Although some observational data has linked daily coffee consumption with decreased incidence of tinnitus, other research suggests that, for modest coffee drinkers (those drinking about 5–10 ounces per day), reducing caffeine intake may reduce tinnitus severity.213,214
Dietary changes are often used as first-line therapies for Ménière disease, a condition that can cause tinnitus.215 A low-salt diet to relieve fluid retention is the most common recommendation, and while it may be helpful in some cases, there is minimal scientific evidence to support it.216,217 Alcohol and caffeine restriction are also frequently recommended, but are similarly lacking in supportive research.215,218 Other speculative interventions include dairy avoidance and a gluten-free diet.33,219
What are Effective Coping Strategies for Living with Tinnitus?
Because chronic tinnitus has no cure, finding effective coping strategies is essential for maintaining quality of life.220 Tinnitus sufferers who passively avoid or deny their condition, as well as those whose goal is to eliminate tinnitus, are likely to be frustrated and feel increased anxiety and distress.220-222 Instead, coping strategies that allow tinnitus to be acknowledged and accepted can lead to a greater ability to adapt to life with the condition.220
It has been suggested that finding a balance between limiting social participation (due to tinnitus discomfort) and spontaneously engaging in enjoyable activities is key to building tolerance.222 In addition, a sense of personal resiliency in the face of negative emotions has been correlated with lower tinnitus-related annoyance, suggesting strategies that build self-resiliency may be helpful to individuals learning to live with tinnitus.223
A wide range of self-help skills have been explored for living with tinnitus. For example, the U.S. Department of Veterans Affairs has developed a progressive treatment approach that employs techniques such as guided imagery, deep breathing, relaxation, and engagement in enjoyable pastimes, and can progress beyond self-help to include cognitive behavioral therapy, sound generators, and other more intensive therapies.224 Researchers have found, among 155 individuals who completed a tinnitus self-management skills training workshop and responded to a follow-up survey six to 10 years later, more than half were still using all of the skills they learned, and relaxation was the most commonly practiced. Approximately 69% of respondents reported they felt more able to control their response to tinnitus, and about half reported improved well-being.225 Another survey study with 460 participants with chronic tinnitus found 40.9% used one or more self-help strategies to reduce their tinnitus severity. In this study, sound therapy was the most commonly used treatment, and other coping practices included diverting attention, relaxation, meditation, yoga, and physical activity.226
9 Tinnitus: Frequently Asked Questions
What does tinnitus sound like?
Tinnitus is often described as “ringing” in the ears, but may also be perceived as buzzing, whistling, hissing, rushing, crackling, beeping, or simply an unpleasant sound.11
Who treats tinnitus?
A primary healthcare provider can help determine whether your tinnitus needs investigation and possibly treatment by an audiologist or other specialist, but many people with tinnitus manage their condition with self-help measures. A psychotherapist or counselor may also be part of a tinnitus healthcare team.12
How long does tinnitus last?
Depending on the cause, tinnitus may resolve quickly or persist for months or years. Chronic tinnitus (lasting three months or longer) usually does not go away, but many people become habituated to their tinnitus, such that is becomes less bothersome over time.20
Does tinnitus cause hearing loss?
Hearing loss is the most common cause of tinnitus, and the two conditions share certain risk factors and mechanisms. However, while tinnitus may cause trouble hearing by obscuring sound, tinnitus does not cause hearing loss.2
Is tinnitus curable?
Chronic tinnitus is considered incurable, but most people with chronic tinnitus improve a small amount over time.19
Is tinnitus dangerous?
Tinnitus is not dangerous. However, it can be a symptom of a dangerous or even life-threatening condition, such as stroke, aneurysm, hemorrhage, or other cardiovascular emergency. Warning signs that tinnitus might be due to a dangerous underlying cause include a pulsating sound, a sudden onset, affecting only one side, or occurring at the same time as other neurological changes.2
Why is tinnitus worse at night?
When tinnitus is worse at night, it may be due to surroundings being quieter and less able to mask the tinnitus sound. Other possible factors include changes in posture and muscle tension, or circadian changes in stress hormone levels.15
What does tinnitus do to your brain?
The brain adapts to tinnitus in various ways, depending on the individual. In some cases, nerve networks between the auditory system and other brain regions are altered by tinnitus, a process that can lead to increased anxiety, depression, and stress. Unfortunately, this is thought to reinforce tinnitus-related nerve signaling and make it harder to recover from tinnitus.75
Can you prevent tinnitus?
Protecting yourself from loud noise at work and in recreational activities, not smoking, and maintaining good heart and general health are ways to lower your risk of tinnitus.4
Disclaimer and Safety Information
This information (and any accompanying material) is not intended to replace the attention or advice of a physician or other qualified health care professional. Anyone who wishes to embark on any dietary, drug, exercise, or other lifestyle change intended to prevent or treat a specific disease or condition should first consult with and seek clearance from a physician or other qualified health care professional. Pregnant women in particular should seek the advice of a physician before using any protocol listed on this website. The protocols described on this website are for adults only, unless otherwise specified. Product labels may contain important safety information and the most recent product information provided by the product manufacturers should be carefully reviewed prior to use to verify the dose, administration, and contraindications. National, state, and local laws may vary regarding the use and application of many of the therapies discussed. The reader assumes the risk of any injuries. The authors and publishers, their affiliates and assigns are not liable for any injury and/or damage to persons arising from this protocol and expressly disclaim responsibility for any adverse effects resulting from the use of the information contained herein.
The protocols raise many issues that are subject to change as new data emerge. None of our suggested protocol regimens can guarantee health benefits. Life Extension has not performed independent verification of the data contained in the referenced materials, and expressly disclaims responsibility for any error in the literature.
- Messina A, Corvaia A, Marino C. Definition of Tinnitus. Audiol Res. May 23 2022;12(3):281-289. doi:10.3390/audiolres12030029. https://www.ncbi.nlm.nih.gov/pubmed/35645199
- Han BI, Lee HW, Ryu S, Kim JS. Tinnitus Update. J Clin Neurol. Jan 2021;17(1):1-10. doi:10.3988/jcn.2021.17.1.1. https://www.ncbi.nlm.nih.gov/pubmed/33480192
- Dinces EA, Deschler DG, (ed.), Lisa Kunins M, (ed.). Patient education: Tinnitus (ringing in the ears) (Beyond the Basics). UpToDate. Updated Oct. 6, 2021. Accessed Apr. 21, 2022, https://www.uptodate.com/contents/tinnitus-ringing-in-the-ears-beyond-the-basics?search=hearing%20loss%20&topicRef=16547&source=see_link
- Simoes JP, Daoud E, Shabbir M, et al. Multidisciplinary Tinnitus Research: Challenges and Future Directions From the Perspective of Early Stage Researchers. Front Aging Neurosci. 2021;13:647285. doi:10.3389/fnagi.2021.647285. https://www.ncbi.nlm.nih.gov/pubmed/34177549
- Bhatt JM, Lin HW, Bhattacharyya N. Prevalence, Severity, Exposures, and Treatment Patterns of Tinnitus in the United States. JAMA Otolaryngol Head Neck Surg . Oct 1 2016;142(10):959-965. doi:10.1001/jamaoto.2016.1700. https://www.ncbi.nlm.nih.gov/pubmed/27441392
- De Ridder D, Vanneste S, Song JJ, Adhia D. Tinnitus and the Triple Network Model: A Perspective. Clin Exp Otorhinolaryngol. Aug 2022;15(3):205-212. doi:10.21053/ceo.2022.00815. https://www.ncbi.nlm.nih.gov/pubmed/35835548
- Joseph AR. Hearing Health Outcomes as a Function of Age, Gender, and Diversity. Semin Hear. Nov 2022;43(4):324-338. doi:10.1055/s-0042-1758377. https://www.ncbi.nlm.nih.gov/pubmed/36466563
- Kreuzer PM, Landgrebe M, Vielsmeier V, Kleinjung T, De Ridder D, Langguth B. Trauma-associated tinnitus. J Head Trauma Rehabil. Sep-Oct 2014;29(5):432-42. doi:10.1097/HTR.0b013e31829d3129. https://www.ncbi.nlm.nih.gov/pubmed/23982788
- Mazurek B, Hesse G, Dobel C, Kratzsch V, Lahmann C, Sattel H, Guideline g. Chronic Tinnitus. Dtsch Arztebl Int. Apr 1 2022;119(13):219-225. doi:10.3238/arztebl.m2022.0135. https://www.ncbi.nlm.nih.gov/pubmed/35197187
- Milinski L, Nodal FR, Vyazovskiy VV, Bajo VM. Tinnitus: at a crossroad between phantom perception and sleep. Brain Commun. 2022;4(3):fcac089. doi:10.1093/braincomms/fcac089. https://www.ncbi.nlm.nih.gov/pubmed/35620170
- Baguley DM, Caimino C, Gilles A, Jacquemin L. The International Vocabulary of Tinnitus. Front Neurosci. 2022;16:887592. doi:10.3389/fnins.2022.887592. https://www.ncbi.nlm.nih.gov/pubmed/35592262
- Dalrymple SN, Lewis SH, Philman S. Tinnitus: Diagnosis and Management. Am Fam Physician. Jun 1 2021;103(11):663-671.
- Coelho CB, Santos R, Campara KF, Tyler R. Classification of Tinnitus: Multiple Causes with the Same Name. Otolaryngol Clin North Am. Aug 2020;53(4):515-529. doi:10.1016/j.otc.2020.03.015. https://www.ncbi.nlm.nih.gov/pubmed/32381342
- Esmaili AA, Renton J. A review of tinnitus. Aust J Gen Pract. Apr 2018;47(4):205-208. doi:10.31128/ajgp-12-17-4420.
- Probst T, Pryss RC, Langguth B, et al. Does Tinnitus Depend on Time-of-Day? An Ecological Momentary Assessment Study with the "TrackYourTinnitus" Application. Front Aging Neurosci. 2017;9:253. doi:10.3389/fnagi.2017.00253. https://www.ncbi.nlm.nih.gov/pubmed/28824415
- Probst T, Pryss R, Langguth B, Schlee W. Emotional states as mediators between tinnitus loudness and tinnitus distress in daily life: Results from the "TrackYourTinnitus" application. Sci Rep. Feb 8 2016;6:20382. doi:10.1038/srep20382. https://www.ncbi.nlm.nih.gov/pubmed/26853815
- Probst T, Pryss R, Langguth B, Schlee W. Emotion dynamics and tinnitus: Daily life data from the "TrackYourTinnitus" application. Sci Rep. Aug 4 2016;6:31166. doi:10.1038/srep31166. https://www.ncbi.nlm.nih.gov/pubmed/27488227
- Vielsmeier V, Santiago Stiel R, Kwok P, Langguth B, Schecklmann M. From Acute to Chronic Tinnitus: Pilot Data on Predictors and Progression. Front Neurol . 2020;11:997. doi:10.3389/fneur.2020.00997. https://www.ncbi.nlm.nih.gov/pubmed/33041971
- Phillips JS, McFerran DJ, Hall DA, Hoare DJ. The natural history of subjective tinnitus in adults: A systematic review and meta-analysis of no-intervention periods in controlled trials. Laryngoscope. Jan 2018;128(1):217-227. doi:10.1002/lary.26607. https://www.ncbi.nlm.nih.gov/pubmed/28425615
- Simoes JP, Neff PKA, Langguth B, Schlee W, Schecklmann M. The progression of chronic tinnitus over the years. Sci Rep. Feb 18 2021;11(1):4162. doi:10.1038/s41598-021-83068-5. https://www.ncbi.nlm.nih.gov/pubmed/33602995
- Folmer RL. Long-term reductions in tinnitus severity. BMC Ear Nose Throat Disord . Sep 16 2002;2(1):3. doi:10.1186/1472-6815-2-3. https://www.ncbi.nlm.nih.gov/pubmed/12234379
- Dawes P, Newall J, Stockdale D, Baguley DM. Natural history of tinnitus in adults: a cross-sectional and longitudinal analysis. BMJ Open. Dec 10 2020;10(12):e041290. doi:10.1136/bmjopen-2020-041290. https://www.ncbi.nlm.nih.gov/pubmed/33303456
- Stouffer JL, Tyler RS. Characterization of tinnitus by tinnitus patients. J Speech Hear Disord. Aug 1990;55(3):439-53. doi:10.1044/jshd.5503.439.
- Kim HJ, Lee HJ, An SY, et al. Analysis of the prevalence and associated risk factors of tinnitus in adults. PLoS One. 2015;10(5):e0127578. doi:10.1371/journal.pone.0127578. https://www.ncbi.nlm.nih.gov/pubmed/26020239
- Auerbach BD, Rodrigues PV, Salvi RJ. Central gain control in tinnitus and hyperacusis. Front Neurol. 2014;5:206. doi:10.3389/fneur.2014.00206. https://www.ncbi.nlm.nih.gov/pubmed/25386157
- Vijayakumar KA, Cho GW, Maharajan N, Jang CH. A Review on Peripheral Tinnitus, Causes, and Treatments from the Perspective of Autophagy. Experimental neurobiology . Aug 31 2022;31(4):232-242. doi:10.5607/en22002. https://www.ncbi.nlm.nih.gov/pubmed/36050223
- Minami SB, Oishi N, Watabe T, Wasano K, Ogawa K. Age-related change of auditory functional connectivity in Human Connectome Project data and tinnitus patients. Laryngoscope Investig Otolaryngol. Feb 2020;5(1):132-136. doi:10.1002/lio2.338. https://www.ncbi.nlm.nih.gov/pubmed/32128439
- Brueggemann P, Neff PKA, Meyer M, Riemer N, Rose M, Mazurek B. On the relationship between tinnitus distress, cognitive performance and aging. Progress in brain research. 2021;262:263-285. doi:10.1016/bs.pbr.2021.01.028. https://www.ncbi.nlm.nih.gov/pubmed/33931184
- Clifford RE, Ryan AF, Program VAMV. The Interrelationship of Tinnitus and Hearing Loss Secondary to Age, Noise Exposure, and Traumatic Brain Injury. Ear Hear. Jul-Aug 01 2022;43(4):1114-1124. doi:10.1097/AUD.0000000000001222. https://www.ncbi.nlm.nih.gov/pubmed/35612496
- Couth S, Mazlan N, Moore DR, Munro KJ, Dawes P. Hearing Difficulties and Tinnitus in Construction, Agricultural, Music, and Finance Industries: Contributions of Demographic, Health, and Lifestyle Factors. Trends Hear . Jan-Dec 2019;23:2331216519885571. doi:10.1177/2331216519885571. https://www.ncbi.nlm.nih.gov/pubmed/31747526
- Goderie T, van Wier MF, Lissenberg-Witte BI, Merkus P, Smits C, Leemans CR, Kramer SE. Factors Associated With the Development of Tinnitus and With the Degree of Annoyance Caused by Newly Developed Tinnitus. Ear Hear. Nov-Dec 01 2022;43(6):1807-1815. doi:10.1097/AUD.0000000000001250. https://www.ncbi.nlm.nih.gov/pubmed/35729718
- Aarhus L, Homoe P, Engdahl B. Otitis Media in Childhood and Disease in Adulthood: A 40-Year Follow-Up Study. Ear Hear. Jan/Feb 2020;41(1):67-71. doi:10.1097/AUD.0000000000000729. https://www.ncbi.nlm.nih.gov/pubmed/30998545
- Oguz E, Cebeci A, Gecici CR. The relationship between nutrition and Meniere's disease. Auris Nasus Larynx. Oct 2021;48(5):803-808. doi:10.1016/j.anl.2021.03.006. https://www.ncbi.nlm.nih.gov/pubmed/33773852
- Lima AF, Moreira FC, Costa IE, Azevedo C, Mar F, Dias L. Tinnitus and Otosclerosis: An Exploratory Study about the Prevalence, Features and Impact in Daily Life. Int Arch Otorhinolaryngol. Jul 2022;26(3):e390-e395. doi:10.1055/s-0041-1739967. https://www.ncbi.nlm.nih.gov/pubmed/35846815
- Fournier P, Paleressompoulle D, Esteve Fraysse MJ, Paolino F, Deveze A, Venail F, Norena A. Exploring the middle ear function in patients with a cluster of symptoms including tinnitus, hyperacusis, ear fullness and/or pain. Hear Res. May 13 2022;422:108519. doi:10.1016/j.heares.2022.108519. https://www.ncbi.nlm.nih.gov/pubmed/35644108
- Zipfel TE, Kaza SR, Greene JS. Middle-ear myoclonus. J Laryngol Otol . Mar 2000;114(3):207-9. doi:10.1258/0022215001905120. https://www.ncbi.nlm.nih.gov/pubmed/10829111
- Hamrang-Yousefi S, Ng J, Andaloro C. Eustachian Tube Dysfunction. StatPearls . StatPearls Publishing Copyright © 2022, StatPearls Publishing LLC.; 2023.
- Salehi PP, Kasle D, Torabi SJ, Michaelides E, Hildrew DM. The etiology, pathogeneses, and treatment of objective tinnitus: Unique case series and literature review. Am J Otolaryngol. Jul-Aug 2019;40(4):594-597. doi:10.1016/j.amjoto.2019.03.017. https://www.ncbi.nlm.nih.gov/pubmed/30981445
- Koparal M, Sirik M, Yavuz GY, Ege B. Evaluation of the relationship between temporomandibular joint disorders and tinnitus with computed tomography. Journal of stomatology, oral and maxillofacial surgery. Sep 2022;123(4):e199-e205. doi:10.1016/j.jormas.2022.06.015. https://www.ncbi.nlm.nih.gov/pubmed/35724865
- Thai NLB, Mai NY, Vuong NL, et al. Treatment for vestibular schwannoma: Systematic review and single arm meta-analysis. Am J Otolaryngol. Mar-Apr 2022;43(2):103337. doi:10.1016/j.amjoto.2021.103337. https://www.ncbi.nlm.nih.gov/pubmed/34973662
- Kumar R, Rice S, Lingam RK. Detecting causes of pulsatile tinnitus on CT arteriography-venography: A pictorial review. European journal of radiology . Jun 2021;139:109722. doi:10.1016/j.ejrad.2021.109722. https://www.ncbi.nlm.nih.gov/pubmed/33894642
- National Guideline C. NICE Evidence Reviews Collection. Evidence review for betahistine: Tinnitus: assessment and management: Evidence review N . National Institute for Health and Care Excellence (NICE) Copyright © NICE 2020.; 2020. NICE Evidence Reviews Collection.
- Patel R, Sabat S, Kanekar S. Imaging Manifestations of Neurologic Complications in Anemia. Hematol Oncol Clin North Am. Aug 2016;30(4):733-56. doi:10.1016/j.hoc.2016.03.002. https://www.ncbi.nlm.nih.gov/pubmed/27443995
- Oosterloo BC, de Feijter M, Croll PH, Baatenburg de Jong RJ, Luik AI, Goedegebure A. Cross-sectional and Longitudinal Associations Between Tinnitus and Mental Health in a Population-Based Sample of Middle-aged and Elderly Persons. JAMA Otolaryngol Head Neck Surg. Aug 1 2021;147(8):708-716. doi:10.1001/jamaoto.2021.1049. https://www.ncbi.nlm.nih.gov/pubmed/34110355
- Stegeman I, Eikelboom RH, Smit AL, et al. Tinnitus and its associations with general health, mental health and hearing loss. Progress in brain research . 2021;262:431-450. doi:10.1016/bs.pbr.2021.01.023. https://www.ncbi.nlm.nih.gov/pubmed/33931190
- Pupic-Bakrac J, Pupic-Bakrac A. Comorbidity of Chronic Tinnitus and Psychological Stress - Which Came First, the Chicken or the Egg? Psychiatr Danub . Nov 2020;32(Suppl 4):412-419. https://www.ncbi.nlm.nih.gov/pubmed/33212444
- Peng J, Dong Y, Luo Y, et al. The Relationship Between Sleep Traits and Tinnitus in UK Biobank: A Population-Based Cohort Study. Ear Hear. Jan-Feb 01 2023;44(1):53-60. doi:10.1097/AUD.0000000000001273. https://www.ncbi.nlm.nih.gov/pubmed/36194023
- Lu CT, Lee LA, Lee GS, Li HY. Obstructive Sleep Apnea and Auditory Dysfunction-Does Snoring Sound Play a Role? Diagnostics (Basel). Sep 30 2022;12(10)doi:10.3390/diagnostics12102374. https://www.ncbi.nlm.nih.gov/pubmed/36292063
- Tsirves GK, Voulgari PV, Pelechas E, Asimakopoulos AD, Drosos AA. Cochlear involvement in patients with systemic autoimmune rheumatic diseases: a clinical and laboratory comparative study. Eur Arch Otorhinolaryngol . Sep 2019;276(9):2419-2426. doi:10.1007/s00405-019-05487-5. https://www.ncbi.nlm.nih.gov/pubmed/31175453
- Sakano H, Harris JP. Emerging options in immune-mediated hearing loss. Laryngoscope Investig Otolaryngol. Feb 2019;4(1):102-108. doi:10.1002/lio2.205. https://www.ncbi.nlm.nih.gov/pubmed/30828626
- Hsu A, Tsou YA, Wang TC, Chang WD, Lin CL, Tyler RS. Hypothyroidism and related comorbidities on the risks of developing tinnitus. Sci Rep. Mar 1 2022;12(1):3401. doi:10.1038/s41598-022-07457-0. https://www.ncbi.nlm.nih.gov/pubmed/35233053
- Garcia A, Madrigal J, Castillo M. Vestibular Migraine and Tinnitus: A Challenging Narrative. Cureus. Jun 2021;13(6):e15998. doi:10.7759/cureus.15998. https://www.ncbi.nlm.nih.gov/pubmed/34336489
- Campello CP, Lemos CAA, Andrade WTL, Melo LPF, Nunes GRS, Cavalcanti HG. Migraine associated with tinnitus and hearing loss in adults: a systematic review. Int J Audiol. Dec 2 2022:1-7. doi:10.1080/14992027.2022.2151943. https://www.ncbi.nlm.nih.gov/pubmed/36459425
- Musleh A, Alshehri S, Qobty A. Hyperlipidemia and its relation with tinnitus: Cross-sectional approach. Nigerian journal of clinical practice . Jul 2022;25(7):1046-1049. doi:10.4103/njcp.njcp_1465_21. https://www.ncbi.nlm.nih.gov/pubmed/35859463
- Avci D. Increased Serum Lipid Levels in Patients with Subjective Tinnitus. Iran J Otorhinolaryngol. Jan 2021;33(114):31-36. doi:10.22038/ijorl.2020.43663.2442. https://www.ncbi.nlm.nih.gov/pubmed/33654688
- Yucel H, Yucel A, Arbag H, Cure E, Eryilmaz MA, Ozer AB. Effect of statins on hearing function and subjective tinnitus in hyperlipidemic patients. Romanian journal of internal medicine = Revue roumaine de medecine interne . Jun 1 2019;57(2):133-140. doi:10.2478/rjim-2018-0035. https://www.ncbi.nlm.nih.gov/pubmed/30447148
- Hameed MK, Sheikh ZA, Ahmed A, Najam A. Atorvastatin in the management of tinnitus with hyperlipidemias. Journal of the College of Physicians and Surgeons--Pakistan : JCPSP . Dec 2014;24(12):927-30. https://www.ncbi.nlm.nih.gov/pubmed/25523730
- Narsinh KH, Hui F, Saloner D, et al. Diagnostic Approach to Pulsatile Tinnitus: A Narrative Review. JAMA Otolaryngol Head Neck Surg. May 1 2022;148(5):476-483. doi:10.1001/jamaoto.2021.4470. https://www.ncbi.nlm.nih.gov/pubmed/35201283
- Wang MTM, Bhatti MT, Danesh-Meyer HV. Idiopathic intracranial hypertension: Pathophysiology, diagnosis and management. J Clin Neurosci. Jan 2022;95:172-179. doi:10.1016/j.jocn.2021.11.029. https://www.ncbi.nlm.nih.gov/pubmed/34929642
- Figueiredo RR, Azevedo AA, Penido NO. Positive Association between Tinnitus and Arterial Hypertension. Front Neurol. 2016;7:171. doi:10.3389/fneur.2016.00171. https://www.ncbi.nlm.nih.gov/pubmed/27761128
- Figueiredo RR, de Azevedo AA, Penido Nde O. Tinnitus and arterial hypertension: a systematic review. Eur Arch Otorhinolaryngol. Nov 2015;272(11):3089-94. doi:10.1007/s00405-014-3277-y. https://www.ncbi.nlm.nih.gov/pubmed/25190255
- Huang PH, Xirasagar S, Chen JH, Cheng YF, Kuo NW, Lin HC. Absence of Association of Tinnitus With Pre-existing Hypertension: A Population-based Study. Ann Otol Rhinol Laryngol. Aug 3 2022:34894221115756. doi:10.1177/00034894221115756. https://www.ncbi.nlm.nih.gov/pubmed/35923124
- Kumar P, Singh NK, Apeksha K, Ghosh V, Kumar RR, Kumar Muthaiah B. Auditory and Vestibular Functioning in Individuals with Type-2 Diabetes Mellitus: A Systematic Review. Int Arch Otorhinolaryngol. Apr 2022;26(2):e281-e288. doi:10.1055/s-0041-1726041. https://www.ncbi.nlm.nih.gov/pubmed/35602282
- Biswas R, Lugo A, Genitsaridi E, et al. Modifiable lifestyle-related risk factors for tinnitus in the general population: An overview of smoking, alcohol, body mass index and caffeine intake. Progress in brain research . 2021;263:1-24. doi:10.1016/bs.pbr.2021.04.005. https://www.ncbi.nlm.nih.gov/pubmed/34243884
- Marchiori LLM, Marchiori GM, Carlos P, Benites SL, Mendes MSB, Ciquinato DSA. Do Body Mass Index Levels Correlate with Tinnitus Among Teachers? Int Arch Otorhinolaryngol. Jan 2022;26(1):e063-e068. doi:10.1055/s-0040-1722251. https://www.ncbi.nlm.nih.gov/pubmed/35096160
- Ozbey-Yucel U, Aydogan Z, Tokgoz-Yilmaz S, Ucar A, Ocak E, Beton S. The effects of diet and physical activity induced weight loss on the severity of tinnitus and quality of life: A randomized controlled trial. Clin Nutr ESPEN . Aug 2021;44:159-165. doi:10.1016/j.clnesp.2021.05.010. https://www.ncbi.nlm.nih.gov/pubmed/34330461
- Ozbey-Yucel U, Ucar A, Aydogan Z, Tokgoz-Yilmaz S, Beton S. The effects of dietary and physical activity interventions on tinnitus symptoms: An RCT. Auris Nasus Larynx. Feb 2023;50(1):40-47. doi:10.1016/j.anl.2022.04.013. https://www.ncbi.nlm.nih.gov/pubmed/35568580
- Hung SH, Xirasagar S, Cheng YF, Kuo NW, Lin HC. Association of Chronic Kidney Disease with Prior Tinnitus: A Case-Control Study. J Clin Med . Dec 19 2022;11(24)doi:10.3390/jcm11247524. https://www.ncbi.nlm.nih.gov/pubmed/36556140
- Krajewska Wojciechowska J, Krajewski W, Zatonski T. Otorhinolaryngological dysfunctions induced by chronic kidney disease in pre- and post-transplant stages. Eur Arch Otorhinolaryngol. Jun 2020;277(6):1575-1591. doi:10.1007/s00405-020-05925-9. https://www.ncbi.nlm.nih.gov/pubmed/32222803
- Boecking B, Klasing S, Walter M, Brueggemann P, Nyamaa A, Rose M, Mazurek B. Vascular-Metabolic Risk Factors and Psychological Stress in Patients with Chronic Tinnitus. Nutrients. May 28 2022;14(11)doi:10.3390/nu14112256. https://www.ncbi.nlm.nih.gov/pubmed/35684056
- ATA. American Tinnitus Association. Measuring Tinnitus. Available at https://www.ata.org/about-tinnitus/patient-tools/measuring-tinnitus/ Accessed 01/10/2023. 2022;
- Vittorini P, Chamoso P, De la Prieta F. A device and an app for the diagnosis and self-management of tinnitus. J Integr Bioinform. Sep 1 2022;19(3)doi:10.1515/jib-2022-0004. https://www.ncbi.nlm.nih.gov/pubmed/36039680
- Altissimi G, Salviati M, Turchetta R, et al. When alarm bells ring: emergency tinnitus. Eur Rev Med Pharmacol Sci. Jul 2016;20(14):2955-73. https://www.ncbi.nlm.nih.gov/pubmed/27460721
- Haider HF, Bojic T, Ribeiro SF, Paco J, Hall DA, Szczepek AJ. Pathophysiology of Subjective Tinnitus: Triggers and Maintenance. Review. Front Neurosci. 2018-November-27 2018;12:866. doi:10.3389/fnins.2018.00866. https://www.ncbi.nlm.nih.gov/pubmed/30538616
- Saeed S, Khan QU. The Pathological Mechanisms and Treatments of Tinnitus. Discoveries (Craiova). Jul-Sep 2021;9(3):e137. doi:10.15190/d.2021.16. https://www.ncbi.nlm.nih.gov/pubmed/35350720
- Shahsavarani S, Schmidt SA, Khan RA, Tai Y, Husain FT. Salience, emotion, and attention: The neural networks underlying tinnitus distress revealed using music and rest. Brain Res. Mar 15 2021;1755:147277. doi:10.1016/j.brainres.2021.147277. https://www.ncbi.nlm.nih.gov/pubmed/33422540
- Folmer RL, Shi BY. Chronic tinnitus resulting from cerumen removal procedures. Int Tinnitus J. 2004;10(1):42-6.
- Michaudet C, Malaty J. Cerumen Impaction: Diagnosis and Management. Am Fam Physician . Oct 15 2018;98(8):525-529. https://www.aafp.org/dam/brand/aafp/pubs/afp/issues/2018/1015/p525.pdf
- Altissimi G, Colizza A, Cianfrone G, et al. Drugs inducing hearing loss, tinnitus, dizziness and vertigo: an updated guide. Eur Rev Med Pharmacol Sci . Aug 2020;24(15):7946-7952. doi:10.26355/eurrev_202008_22477. https://www.ncbi.nlm.nih.gov/pubmed/32767320
- Curhan SG, Glicksman J, Wang M, Eavey RD, Curhan GC. Longitudinal Study of Analgesic Use and Risk of Incident Persistent Tinnitus. J Gen Intern Med . Nov 2022;37(14):3653-3662. doi:10.1007/s11606-021-07349-5. https://www.ncbi.nlm.nih.gov/pubmed/35132561
- Kim SH, Kim D, Lee JM, Lee SK, Kang HJ, Yeo SG. Review of Pharmacotherapy for Tinnitus. Healthcare (Basel, Switzerland). Jun 21 2021;9(6)doi:10.3390/healthcare9060779. https://www.ncbi.nlm.nih.gov/pubmed/34205776
- De Luca P, Scarpa A, De Bonis E, et al. Chloroquine and hydroxychloroquine ototoxicity; potential implications for SARS-CoV-2 treatment. A brief review of the literature. Am J Otolaryngol. Sep-Oct 2021;42(5):102640. doi:10.1016/j.amjoto.2020.102640. https://www.ncbi.nlm.nih.gov/pubmed/33780902
- Mitre EI, Figueira AS, Rocha AB, Alves SM. Audiometric and vestibular evaluation in women using the hormonal contraceptive method. Braz J Otorhinolaryngol . May-Jun 2006;72(3):350-4. doi:10.1016/s1808-8694(15)30967-8. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9443595/pdf/main.pdf
- Pienkowski M. Loud Music and Leisure Noise Is a Common Cause of Chronic Hearing Loss, Tinnitus and Hyperacusis. Int J Environ Res Public Health . Apr 16 2021;18(8)doi:10.3390/ijerph18084236. https://www.ncbi.nlm.nih.gov/pubmed/33923580
- Gopal KV, Mills LE, Phillips BS, Nandy R. Risk Assessment of Recreational Noise-Induced Hearing Loss from Exposure through a Personal Audio System-iPod Touch. J Am Acad Audiol. Jul/Aug 2019;30(7):619-633. doi:10.3766/jaaa.17140. https://www.ncbi.nlm.nih.gov/pubmed/30395532
- Jiang W, Zhao F, Guderley N, Manchaiah V. Daily music exposure dose and hearing problems using personal listening devices in adolescents and young adults: A systematic review. Int J Audiol. 2016;55(4):197-205. doi:10.3109/14992027.2015.1122237. https://www.ncbi.nlm.nih.gov/pubmed/26768911
- NIOSH. National Institute for Occupational Safety and Health: Noise & Hearing Loss Prevention. Available at https://www.cdc.gov/niosh/topics/noise/default.html Last updated 02/06/2018. Accessed 01/25/2023. 2018;
- Barth SW, Lehner MD, Dietz GPH, Schulze H. Pharmacologic treatments in preclinical tinnitus models with special focus on Ginkgo biloba leaf extract EGb 761(R). Molecular and cellular neurosciences. Oct 2021;116:103669. doi:10.1016/j.mcn.2021.103669. https://www.ncbi.nlm.nih.gov/pubmed/34560255
- Krauss P, Tziridis K, Buerbank S, Schilling A, Schulze H. Therapeutic Value of Ginkgo biloba Extract EGb 761(R) in an Animal Model (Meriones unguiculatus) for Noise Trauma Induced Hearing Loss and Tinnitus. PLoS One . 2016;11(6):e0157574. doi:10.1371/journal.pone.0157574. https://www.ncbi.nlm.nih.gov/pubmed/27315063
- Radunz CL, Okuyama CE, Branco-Barreiro FCA, Pereira RMS, Diniz SN. Clinical randomized trial study of hearing aids effectiveness in association with Ginkgo biloba extract (EGb 761) on tinnitus improvement. Braz J Otorhinolaryngol . Nov-Dec 2020;86(6):734-742. doi:10.1016/j.bjorl.2019.05.003. https://www.ncbi.nlm.nih.gov/pubmed/31300303 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9422696/pdf/main.pdf
- Nishad RK, Jain AK, Singh M, Verma R, Jain S. Randomised Controlled Clinical Study of Injection Caroverine and Ginkgo Biloba Extract in Cochlear Synaptic Tinnitus. Indian journal of otolaryngology and head and neck surgery : official publication of the Association of Otolaryngologists of India . Nov 2019;71(Suppl 2):1523-1528. doi:10.1007/s12070-019-01655-5. https://www.ncbi.nlm.nih.gov/pubmed/31750210 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6841866/pdf/12070_2019_Article_1655.pdf
- Orhan I, Aydin S, Altin G, Yilmaz F. [An efficacy comparison of betahistin, trimetazidine and ginkgo biloba extract in patients with tinnitus]. Kulak Burun Bogaz Ihtis Derg . May-Jun 2013;23(3):143-7. Tinnituslu hastalarda trimetazidin, betahistin ve ginkgo biloba ekstresi etkinliginin karsilastirilmasi. doi:10.5606/kbbihtisas.2013.03064. https://www.ncbi.nlm.nih.gov/pubmed/23682937
- Mahmoudian-Sani MR, Hashemzadeh-Chaleshtori M, Asadi-Samani M, Yang Q. Ginkgo biloba in the treatment of tinnitus: An updated literature review. Int Tinnitus J. Jun 1 2017;21(1):58-62. doi:10.5935/0946-5448.20170011. https://www.ncbi.nlm.nih.gov/pubmed/28723603
- Rejali D, Sivakumar A, Balaji N. Ginkgo biloba does not benefit patients with tinnitus: a randomized placebo-controlled double-blind trial and meta-analysis of randomized trials. Clin Otolaryngol Allied Sci. Jun 2004;29(3):226-31. doi:10.1111/j.1365-2273.2004.00814.x. https://www.ncbi.nlm.nih.gov/pubmed/15142066
- Kramer F, Ortigoza A. Ginkgo biloba for the treatment of tinnitus. Medwave . Oct 17 2018;18(6):e7295. Ginkgo biloba para el tratamiento del tinnitus. doi:10.5867/medwave.2018.06.7294. https://www.ncbi.nlm.nih.gov/pubmed/30339143
- Spiegel R, Kalla R, Mantokoudis G, Maire R, Mueller H, Hoerr R, Ihl R. Ginkgo biloba extract EGb 761((R)) alleviates neurosensory symptoms in patients with dementia: a meta-analysis of treatment effects on tinnitus and dizziness in randomized, placebo-controlled trials. Clin Interv Aging . 2018;13:1121-1127. doi:10.2147/CIA.S157877. https://www.ncbi.nlm.nih.gov/pubmed/29942120
- Bruggemann P, Soria MG, Brandes-Schramm J, Mazurek B. The Influence of Depression, Anxiety and Cognition on the Treatment Effects of Ginkgo biloba Extract EGb 761((R)) in Patients with Tinnitus and Dementia: A Mediation Analysis. J Clin Med. Jul 16 2021;10(14)doi:10.3390/jcm10143151. https://www.ncbi.nlm.nih.gov/pubmed/34300317
- Chen HL, Tan CT, Wu CC, Liu TC. Effects of Diet and Lifestyle on Audio-Vestibular Dysfunction in the Elderly: A Literature Review. Nutrients . Nov 8 2022;14(22)doi:10.3390/nu14224720. https://mdpi-res.com/d_attachment/nutrients/nutrients-14-04720/article_deploy/nutrients-14-04720-v3.pdf?version=1668768942
- Luetzenberg FS, Babu S, Seidman MD. Alternative Treatments of Tinnitus: Alternative Medicine. Otolaryngol Clin North Am. Aug 2020;53(4):637-650. doi:10.1016/j.otc.2020.03.011. https://www.ncbi.nlm.nih.gov/pubmed/32362562
- Repova K, Baka T, Krajcirovicova K, Stanko P, Aziriova S, Reiter RJ, Simko F. Melatonin as a Potential Approach to Anxiety Treatment. Int J Mol Sci . Dec 19 2022;23(24)doi:10.3390/ijms232416187. https://www.ncbi.nlm.nih.gov/pubmed/36555831
- Reiter RJ, Tan DX, Korkmaz A, Fuentes-Broto L. Drug-mediated ototoxicity and tinnitus: alleviation with melatonin. J Physiol Pharmacol. Apr 2011;62(2):151-7. https://www.ncbi.nlm.nih.gov/pubmed/21673362
- Lasisi AO, Fehintola FA, Lasisi TJ. The role of plasma melatonin and vitamins C and B12 in the development of idiopathic tinnitus in the elderly. Ghana Med J. Sep 2012;46(3):152-7. https://www.ncbi.nlm.nih.gov/pubmed/23661829
- Miroddi M, Bruno R, Galletti F, Calapai F, Navarra M, Gangemi S, Calapai G. Clinical pharmacology of melatonin in the treatment of tinnitus: a review. Eur J Clin Pharmacol. Mar 2015;71(3):263-70. doi:10.1007/s00228-015-1805-3. https://www.ncbi.nlm.nih.gov/pubmed/25597877
- Abtahi SH, Hashemi SM, Mahmoodi M, Nilforoush MH. Comparison of Melatonin and Sertraline Therapies on Tinnitus: A Randomized Clinical Trial. International journal of preventive medicine . 2017;8:61. doi:10.4103/ijpvm.IJPVM_229_17. https://www.ncbi.nlm.nih.gov/pubmed/28966750
- Albu S, Chirtes F. Intratympanic dexamethasone plus melatonin versus melatonin only in the treatment of unilateral acute idiopathic tinnitus. Am J Otolaryngol. Sep-Oct 2014;35(5):617-22. doi:10.1016/j.amjoto.2014.06.009. https://www.ncbi.nlm.nih.gov/pubmed/25066140
- Carroll BJ, Piazza G, Goldhaber SZ. Sulodexide in venous disease. J Thromb Haemost . Jan 2019;17(1):31-38. doi:10.1111/jth.14324. https://www.ncbi.nlm.nih.gov/pubmed/30394690
- Ferrari G, Agnese A, Cavallero A, Delehaye E, Rocchetti O, Rossi W, Tombolini A. Medical and surgical treatments for tinnitus: the efficacy of combined treatment with sulodexide and melatonin. Journal of neurosurgical sciences . Mar 2015;59(1):1-9. https://www.ncbi.nlm.nih.gov/pubmed/25413777
- Neri G, De Stefano A, Baffa C, et al. Treatment of central and sensorineural tinnitus with orally administered Melatonin and Sulodexide: personal experience from a randomized controlled study. Acta Otorhinolaryngol Ital . Apr 2009;29(2):86-91. https://www.ncbi.nlm.nih.gov/pubmed/20111618
- Rajesh K, Khan MI, Mahesh P, Kumar SR, Kumar SS. Preclinical and Clinical Role of Coenzyme Q10 Supplementation in Various Pathological States. Drug research . Sep 2022;72(7):367-371. doi:10.1055/a-1835-1738. https://www.ncbi.nlm.nih.gov/pubmed/35724675
- Khan M, Gross J, Haupt H, et al. A pilot clinical trial of the effects of coenzyme Q10 on chronic tinnitus aurium. Otolaryngol Head Neck Surg . Jan 2007;136(1):72-7. doi:10.1016/j.otohns.2006.07.010. https://www.ncbi.nlm.nih.gov/pubmed/17210337 https://journals.sagepub.com/doi/10.1016/j.otohns.2006.07.010?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub 0pubmed
- Fetoni AR, De Bartolo P, Eramo SL, et al. Noise-induced hearing loss (NIHL) as a target of oxidative stress-mediated damage: cochlear and cortical responses after an increase in antioxidant defense. J Neurosci. Feb 27 2013;33(9):4011-23. doi:10.1523/JNEUROSCI.2282-12.2013. https://www.ncbi.nlm.nih.gov/pubmed/23447610
- Staffa P, Cambi J, Mezzedimi C, Passali D, Bellussi L. Activity of coenzyme Q 10 (Q-Ter multicomposite) on recovery time in noise-induced hearing loss. Noise & health. Sep-Oct 2014;16(72):265-9. doi:10.4103/1463-1741.140499. https://www.ncbi.nlm.nih.gov/pubmed/25209035 https://www.noiseandhealth.org/article.asp?issn=1463-1741;year=2014;volume=16;issue=72;spage=265;epage=269;aulast=Staffa
- Scasso F, Sprio AE, Canobbio L, Scanarotti C, Manini G, Berta GN, Bassi AM. Dietary supplementation of coenzyme Q10 plus multivitamins to hamper the ROS mediated cisplatin ototoxicity in humans: A pilot study. Heliyon . Feb 2017;3(2):e00251. doi:10.1016/j.heliyon.2017.e00251. https://www.ncbi.nlm.nih.gov/pubmed/28239674
- Coelho CB, Tyler R, Hansen M. Zinc as a possible treatment for tinnitus. Progress in brain research. 2007;166:279-85. doi:10.1016/S0079-6123(07)66026-9. https://www.ncbi.nlm.nih.gov/pubmed/17956792
- Vogler NW, Betti VM, Goldberg JM, Tzounopoulos T. Mechanisms Underlying Long-Term Synaptic Zinc Plasticity at Mouse Dorsal Cochlear Nucleus Glutamatergic Synapses. J Neurosci. Jun 24 2020;40(26):4981-4996. doi:10.1523/JNEUROSCI.0175-20.2020. https://www.ncbi.nlm.nih.gov/pubmed/32434779
- Berkiten G, Kumral TL, Yildirim G, Salturk Z, Uyar Y, Atar Y. Effects of serum zinc level on tinnitus. Am J Otolaryngol. Mar-Apr 2015;36(2):230-4. doi:10.1016/j.amjoto.2014.11.001. https://www.ncbi.nlm.nih.gov/pubmed/25554004
- Narayanan SS, Murali M, Lucas JC, Sykes KJ. Micronutrients in tinnitus: A National Health and Nutrition Examination Survey analysis. Am J Otolaryngol . May-Jun 2022;43(3):103460. doi:10.1016/j.amjoto.2022.103460. https://www.ncbi.nlm.nih.gov/pubmed/35429847
- Jun HJ, Ok S, Tyler R, Hwang SY, Chae S. Is Hypozincemia Related to Tinnitus?: A Population Study Using Data From the Korea National Health and Nutrition Examination Survey. Clin Exp Otorhinolaryngol. Dec 2015;8(4):335-8. doi:10.3342/ceo.2015.8.4.335. https://www.ncbi.nlm.nih.gov/pubmed/26622950
- Yeh CW, Tseng LH, Yang CH, Hwang CF. Effects of oral zinc supplementation on patients with noise-induced hearing loss associated tinnitus: A clinical trial. Biomedical journal. Feb 2019;42(1):46-52. doi:10.1016/j.bj.2018.10.009. https://www.ncbi.nlm.nih.gov/pubmed/30987704
- Arda HN, Tuncel U, Akdogan O, Ozluoglu LN. The role of zinc in the treatment of tinnitus. Otol Neurotol. Jan 2003;24(1):86-9. doi:10.1097/00129492-200301000-00018. https://www.ncbi.nlm.nih.gov/pubmed/12544035
- Yetiser S, Tosun F, Satar B, Arslanhan M, Akcam T, Ozkaptan Y. The role of zinc in management of tinnitus. Auris Nasus Larynx. Oct 2002;29(4):329-33. doi:10.1016/s0385-8146(02)00023-8. https://www.ncbi.nlm.nih.gov/pubmed/12393036
- Paaske PB, Pedersen CB, Kjems G, Sam IL. Zinc in the management of tinnitus. Placebo-controlled trial. Ann Otol Rhinol Laryngol. Aug 1991;100(8):647-9. doi:10.1177/000348949110000809. https://www.ncbi.nlm.nih.gov/pubmed/1872515
- Paaske PB, Pedersen CB, Kjems G, Sam IL. [Zinc therapy of tinnitus. A placebo-controlled study]. Ugeskrift for laeger. Aug 27 1990;152(35):2473-5. Zinkbehandling af tinnitus. En placebokontrolleret undersogelse. https://www.ncbi.nlm.nih.gov/pubmed/2205961
- Kisli M, Sacmaci H. Auditory Brainstem Response in Patients with Tinnitus Associated with Vitamin B12 Deficiency. Acta Neurol Taiwan. Sep 15 2019;28(3):59-65. https://www.ncbi.nlm.nih.gov/pubmed/32002975
- Dawes P, Cruickshanks KJ, Marsden A, Moore DR, Munro KJ. Relationship Between Diet, Tinnitus, and Hearing Difficulties. Ear Hear. Mar/Apr 2020;41(2):289-299. doi:10.1097/AUD.0000000000000765. https://www.ncbi.nlm.nih.gov/pubmed/31356390
- Shemesh Z, Attias J, Ornan M, Shapira N, Shahar A. Vitamin B12 deficiency in patients with chronic-tinnitus and noise-induced hearing loss. Am J Otolaryngol . Mar-Apr 1993;14(2):94-9. doi:10.1016/0196-0709(93)90046-a. https://www.ncbi.nlm.nih.gov/pubmed/8484483
- Singh C, Kawatra R, Gupta J, Awasthi V, Dungana H. Therapeutic role of Vitamin B12 in patients of chronic tinnitus: A pilot study. Noise & health . Mar-Apr 2016;18(81):93-7. doi:10.4103/1463-1741.178485. https://www.ncbi.nlm.nih.gov/pubmed/26960786
- Hameed HM, Eleue AH, Al Mosawi AMT. The use of distortion product otoacoustic emissions (DPOAE) records to estimate effect of vitamin B complex on changing severity of tinnitus. Ann Med Surg (Lond). Dec 2018;36:203-211. doi:10.1016/j.amsu.2018.10.035. https://www.ncbi.nlm.nih.gov/pubmed/30519463
- Berkiten G, Yildirim G, Topaloglu I, Ugras H. Vitamin B12 levels in patients with tinnitus and effectiveness of vitamin B12 treatment on hearing threshold and tinnitus. B-ent. 2013;9(2):111-6.
- Ratan ZA, Haidere MF, Hong YH, Park SH, Lee JO, Lee J, Cho JY. Pharmacological potential of ginseng and its major component ginsenosides. J Ginseng Res. Mar 2021;45(2):199-210. doi:10.1016/j.jgr.2020.02.004. https://www.ncbi.nlm.nih.gov/pubmed/33841000
- Kim TS, Lee HS, Chung JW. The Effect of Korean Red Ginseng on Symptoms and Quality of Life in Chronic Tinnitus: A Randomized, Open-Label Pilot Study. J Audiol Otol. Sep 2015;19(2):85-90. doi:10.7874/jao.2015.19.2.85. https://www.ncbi.nlm.nih.gov/pubmed/26413574
- Grossi MG, Belcaro G, Cesarone MR, et al. Improvement in cochlear flow with Pycnogenol(R) in patients with tinnitus: a pilot evaluation. Panminerva Med . Jun 2010;52(2 Suppl 1):63-7. https://www.ncbi.nlm.nih.gov/pubmed/20657537
- Luzzi R, Belcaro G, Hu S, et al. Improvement in symptoms and cochlear flow with pycnogenol in patients with Meniere's disease and tinnitus. Minerva Med . Jun 2014;105(3):245-54. https://www.ncbi.nlm.nih.gov/pubmed/24988090
- Kirkland AE, Sarlo GL, Holton KF. The Role of Magnesium in Neurological Disorders. Nutrients. Jun 6 2018;10(6)doi:10.3390/nu10060730. https://www.ncbi.nlm.nih.gov/pubmed/29882776
- Tangvoraphonkchai K, Davenport A. Magnesium and Cardiovascular Disease. Adv Chronic Kidney Dis. May 2018;25(3):251-260. doi:10.1053/j.ackd.2018.02.010. https://www.ncbi.nlm.nih.gov/pubmed/29793664
- Henaut L, Massy ZA. Magnesium as a Calcification Inhibitor. Adv Chronic Kidney Dis . May 2018;25(3):281-290. doi:10.1053/j.ackd.2017.12.001. https://www.ncbi.nlm.nih.gov/pubmed/29793668
- Uluyol S, Kilicaslan S, Yagiz O. Relationship between serum magnesium level and subjective tinnitus. Kulak Burun Bogaz Ihtis Derg. Jul-Aug 2016;26(4):225-7. doi:10.5606/kbbihtisas.2016.87094. https://www.ncbi.nlm.nih.gov/pubmed/27405078
- Cevette MJ, Barrs DM, Patel A, et al. Phase 2 study examining magnesium-dependent tinnitus. Int Tinnitus J. 2011;16(2):168-73. https://www.ncbi.nlm.nih.gov/pubmed/22249877
- Plantone D, Primiano G, Manco C, Locci S, Servidei S, De Stefano N. Vitamin D in Neurological Diseases. Int J Mol Sci. Dec 21 2022;24(1)doi:10.3390/ijms24010087. https://www.ncbi.nlm.nih.gov/pubmed/36613531
- Nowaczewska M, Osinski S, Marzec M, Wicinski M, Bilicka K, Kazmierczak W. The role of vitamin D in subjective tinnitus-A case-control study. PLoS One . 2021;16(8):e0255482. doi:10.1371/journal.pone.0255482. https://www.ncbi.nlm.nih.gov/pubmed/34407088
- Nocini R, Henry BM, Mattiuzzi C, Lippi G. Serum Vitamin D Concentration Is Lower in Patients with Tinnitus: A Meta-Analysis of Observational Studies. Article. Diagnostics (Basel). Mar 8 2023;13(6):1037. doi:10.3390/diagnostics13061037. https://www.ncbi.nlm.nih.gov/pubmed/36980345
- Oppitz SJ, Garcia MV, Bruno RS, et al. Supplementation with acai (Euterpe Oleracea Martius) for the treatment of chronic tinnitus: effects on perception, anxiety levels and oxidative metabolism biomarkers. Codas . 2022;34(4):e20210076. Suplementacao com acai (Euterpe Oleracea Martius) para o tratamento do zumbido cronico: efeitos na percepcao, niveis de ansiedade e biomarcadores de metabolismo oxidativo. doi:10.1590/2317-1782/20212021076. https://www.ncbi.nlm.nih.gov/pubmed/35107519
- Bae M, Ahmed K, Yim JE. Beneficial Effects of Taurine on Metabolic Parameters in Animals and Humans. J Obes Metab Syndr. Jun 30 2022;31(2):134-146. doi:10.7570/jomes21088. https://www.ncbi.nlm.nih.gov/pubmed/35670160
- Jakaria M, Azam S, Haque ME, Jo SH, Uddin MS, Kim IS, Choi DK. Taurine and its analogs in neurological disorders: Focus on therapeutic potential and molecular mechanisms. Redox Biol. Jun 2019;24:101223. doi:10.1016/j.redox.2019.101223. https://www.ncbi.nlm.nih.gov/pubmed/31141786
- Lee AC, Godfrey DA. Cochlear damage affects neurotransmitter chemistry in the central auditory system. Front Neurol. 2014;5:227. doi:10.3389/fneur.2014.00227. https://www.ncbi.nlm.nih.gov/pubmed/25477858
- Tan Y, Lu C, Jiang M, et al. Exploring pathogenesis in subjects with subjective Tinnitus having kidney deficiency pattern in terms of Traditional Chinese Medicine based on serum metabolic profiles. J Tradit Chin Med . Oct 2018;38(5):773-780. https://www.ncbi.nlm.nih.gov/pubmed/32185996
- Rak K, Volker J, Jurgens L, et al. Neurotrophic effects of taurine on spiral ganglion neurons in vitro. Neuroreport. Nov 12 2014;25(16):1250-4. doi:10.1097/WNR.0000000000000254. https://www.ncbi.nlm.nih.gov/pubmed/25202928
- Ye HB, Wang J, Zhang WT, Shi HB, Yin SK. Taurine attenuates bilirubin-induced neurotoxicity in the auditory system in neonatal guinea pigs. Int J Pediatr Otorhinolaryngol. May 2013;77(5):647-54. doi:10.1016/j.ijporl.2012.11.037. https://www.ncbi.nlm.nih.gov/pubmed/23273639
- Godfrey DA, Kaltenbach JA, Chen K, et al. Amino acid concentrations in the hamster central auditory system and long-term effects of intense tone exposure. Journal of neuroscience research. Nov 2012;90(11):2214-24. doi:10.1002/jnr.23095. https://onlinelibrary.wiley.com/doi/10.1002/jnr.23095
- Brozoski TJ, Caspary DM, Bauer CA, Richardson BD. The effect of supplemental dietary taurine on tinnitus and auditory discrimination in an animal model. Hear Res. Dec 1 2010;270(1-2):71-80. doi:10.1016/j.heares.2010.09.006. https://www.ncbi.nlm.nih.gov/pubmed/20868734
- Chen JJ, Chen YW, Zeng BY, et al. Efficacy of pharmacologic treatment in tinnitus patients without specific or treatable origin: A network meta-analysis of randomised controlled trials. EClinicalMedicine. Sep 2021;39:101080. doi:10.1016/j.eclinm.2021.101080. https://www.ncbi.nlm.nih.gov/pubmed/34611615
- Pawlak-Osinska K, Kazmierczak H, Marzec M, et al. Assessment of the State of the Natural Antioxidant Barrier of a Body in Patients Complaining about the Presence of Tinnitus. Oxid Med Cell Longev. 2018;2018:1439575. doi:10.1155/2018/1439575. https://www.ncbi.nlm.nih.gov/pubmed/30510615
- Celik M, Koyuncu I. A Comprehensive Study of Oxidative Stress in Tinnitus Patients. Indian journal of otolaryngology and head and neck surgery : official publication of the Association of Otolaryngologists of India . Dec 2018;70(4):521-526. doi:10.1007/s12070-018-1464-7. https://www.ncbi.nlm.nih.gov/pubmed/30464909
- Song A, Cho GW, Moon C, Park I, Jang CH. Protective Effect of Resveratrol in an Experimental Model of Salicylate-Induced Tinnitus. Int J Mol Sci . Nov 16 2022;23(22)doi:10.3390/ijms232214183. https://www.ncbi.nlm.nih.gov/pubmed/36430660
- Petridou AI, Zagora ET, Petridis P, et al. The Effect of Antioxidant Supplementation in Patients with Tinnitus and Normal Hearing or Hearing Loss: A Randomized, Double-Blind, Placebo Controlled Trial. Nutrients . Dec 12 2019;11(12)doi:10.3390/nu11123037. https://www.ncbi.nlm.nih.gov/pubmed/31842394
- Savastano M, Brescia G, Marioni G. Antioxidant therapy in idiopathic tinnitus: preliminary outcomes. Arch Med Res. May 2007;38(4):456-9. doi:10.1016/j.arcmed.2006.12.004. https://www.ncbi.nlm.nih.gov/pubmed/17416295
- Polanski JF, Soares AD, de Mendonca Cruz OL. Antioxidant therapy in the elderly with tinnitus. Braz J Otorhinolaryngol. May-Jun 2016;82(3):269-74. doi:10.1016/j.bjorl.2015.04.016. https://www.ncbi.nlm.nih.gov/pubmed/26547700
- Knapper J, Girauta MV, Coromina J. Effectiveness of Tinnitan Duo(R) in Subjective Tinnitus with Emotional Affectation: A Prospective, Interventional Study. J Diet Suppl. 2023;20(1):1-14. doi:10.1080/19390211.2021.1944947. https://www.ncbi.nlm.nih.gov/pubmed/34219601
- Curtis F, Laparidou D, Bridle C, et al. Effects of cognitive behavioural therapy on insomnia in adults with tinnitus: Systematic review and meta-analysis of randomised controlled trials. Sleep Med Rev. Apr 2021;56:101405. doi:10.1016/j.smrv.2020.101405. https://www.ncbi.nlm.nih.gov/pubmed/33360841
- Boecking B, Rose M, Brueggemann P, Mazurek B. Two birds with one stone.-Addressing depressive symptoms, emotional tension and worry improves tinnitus-related distress and affective pain perceptions in patients with chronic tinnitus. PLoS One. 2021;16(3):e0246747. doi:10.1371/journal.pone.0246747. https://www.ncbi.nlm.nih.gov/pubmed/33705407
- McKenna L, Vogt F, Marks E. Current Validated Medical Treatments for Tinnitus: Cognitive Behavioral Therapy. Otolaryngol Clin North Am. Aug 2020;53(4):605-615. doi:10.1016/j.otc.2020.03.007. https://www.ncbi.nlm.nih.gov/pubmed/32334871
- Fuller T, Cima R, Langguth B, Mazurek B, Vlaeyen JW, Hoare DJ. Cognitive behavioural therapy for tinnitus. Cochrane Database Syst Rev. Jan 8 2020;1(1):CD012614. doi:10.1002/14651858.CD012614.pub2. https://www.ncbi.nlm.nih.gov/pubmed/31912887
- Kikidis D, Vassou E, Markatos N, Schlee W, Iliadou E. Hearing Aid Fitting in Tinnitus: A Scoping Review of Methodological Aspects and Effect on Tinnitus Distress and Perception. J Clin Med. Jun 29 2021;10(13)doi:10.3390/jcm10132896. https://www.ncbi.nlm.nih.gov/pubmed/34209732
- Suzuki N, Shinden S, Oishi N, Ueno M, Suzuki D, Ogawa K, Ozawa H. Effectiveness of hearing aids in treating patients with chronic tinnitus with average hearing levels of <30 dBHL and no inconvenience due to hearing loss. Acta Otolaryngol. Aug 2021;141(8):773-779. doi:10.1080/00016489.2021.1957145. https://www.ncbi.nlm.nih.gov/pubmed/34369276
- Jastreboff PJ. 25 years of tinnitus retraining therapy. HNO. Apr 2015;63(4):307-11. doi:10.1007/s00106-014-2979-1. https://www.ncbi.nlm.nih.gov/pubmed/25862626
- Han M, Yang X, Lv J. Efficacy of tinnitus retraining therapy in the treatment of tinnitus: A meta-analysis and systematic review. Am J Otolaryngol . Nov-Dec 2021;42(6):103151. doi:10.1016/j.amjoto.2021.103151. https://www.ncbi.nlm.nih.gov/pubmed/34303210
- Tinnitus Retraining Therapy Trial Research G, Scherer RW, Formby C. Effect of Tinnitus Retraining Therapy vs Standard of Care on Tinnitus-Related Quality of Life: A Randomized Clinical Trial. JAMA Otolaryngol Head Neck Surg . Jul 1 2019;145(7):597-608. doi:10.1001/jamaoto.2019.0821. https://www.ncbi.nlm.nih.gov/pubmed/31120533
- Okamoto H, Stracke H, Stoll W, Pantev C. Listening to tailor-made notched music reduces tinnitus loudness and tinnitus-related auditory cortex activity. Proc Natl Acad Sci U S A. Jan 19 2010;107(3):1207-10. doi:10.1073/pnas.0911268107. https://www.ncbi.nlm.nih.gov/pubmed/20080545
- Pape J, Paraskevopoulos E, Bruchmann M, Wollbrink A, Rudack C, Pantev C. Playing and listening to tailor-made notched music: cortical plasticity induced by unimodal and multimodal training in tinnitus patients. Neural plasticity . 2014;2014:516163. doi:10.1155/2014/516163. https://www.ncbi.nlm.nih.gov/pubmed/24895541
- Schad ML, McMillan GP, Thielman EJ, Groon K, Morse-Fortier C, Martin JL, Henry JA. Comparison of acoustic therapies for tinnitus suppression: a preliminary trial. Int J Audiol. Feb 2018;57(2):143-149. doi:10.1080/14992027.2017.1385862. https://www.ncbi.nlm.nih.gov/pubmed/29022411
- Peter N, Kleinjung T. Neuromodulation for tinnitus treatment: an overview of invasive and non-invasive techniques. Journal of Zhejiang University Science B . Feb. 2019;20(2):116-130. doi:10.1631/jzus.B1700117. https://www.ncbi.nlm.nih.gov/pubmed/29770647
- Denton AJ, Finberg A, Ashman PE, et al. Implications of Transcranial Magnetic Stimulation as a Treatment Modality for Tinnitus. J Clin Med . Nov 20 2021;10(22)doi:10.3390/jcm10225422. https://www.ncbi.nlm.nih.gov/pubmed/34830704
- Lefebvre-Demers M, Doyon N, Fecteau S. Non-invasive neuromodulation for tinnitus: A meta-analysis and modeling studies. Brain Stimul. Jan-Feb 2021;14(1):113-128. doi:10.1016/j.brs.2020.11.014. https://www.ncbi.nlm.nih.gov/pubmed/33276156
- Yin L, Chen X, Lu X, An Y, Zhang T, Yan J. An updated meta-analysis: repetitive transcranial magnetic stimulation for treating tinnitus. J Int Med Res . Mar 2021;49(3):300060521999549. doi:10.1177/0300060521999549. https://www.ncbi.nlm.nih.gov/pubmed/33729855
- Sobreira G, Aleixo MA, Moreia C, Oliveira J. Adverse effects in repetitive transcranial magnetic stimulation – prevention and management. European Psychiatry . 2016/03/01/ 2020;33(S1):S555-S556. doi:10.1016/j.eurpsy.2016.01.2052. https://www.sciencedirect.com/science/article/pii/S0924933816020563 https://www.cambridge.org/core/journals/european-psychiatry/article/abs/adverse-effects-in-repetitive-transcranial-magnetic-stimulation-prevention-and-management/C8E83ED8E307F6265215BAD29BA48FF6
- Liang Z, Yang H, Cheng G, Huang L, Zhang T, Jia H. Repetitive transcranial magnetic stimulation on chronic tinnitus: a systematic review and meta-analysis. BMC Psychiatry. Nov 23 2020;20(1):547. doi:10.1186/s12888-020-02947-9. https://www.ncbi.nlm.nih.gov/pubmed/33228598
- Hoare DJ, Adjamian P, Sereda M. Electrical Stimulation of the Ear, Head, Cranial Nerve, or Cortex for the Treatment of Tinnitus: A Scoping Review. Neural plasticity. 2016;2016:5130503. doi:10.1155/2016/5130503. https://www.ncbi.nlm.nih.gov/pubmed/27403346
- Yang T, Zhang J, Wang B, Zhang W, Xu M, Yang S, Liu H. Electrical stimulation to treat tinnitus: a meta-analysis and systemic review of randomized controlled trials. Therapeutic advances in chronic disease . 2021;12:20406223211041069. doi:10.1177/20406223211041069. https://www.ncbi.nlm.nih.gov/pubmed/34729140
- Martins ML, Souza DDS, Cavalcante M, et al. Effect of transcranial Direct Current Stimulation for tinnitus treatment: A systematic review and meta-analysis. Neurophysiol Clin. Feb 2022;52(1):1-16. doi:10.1016/j.neucli.2021.12.005. https://www.ncbi.nlm.nih.gov/pubmed/35027291
- Byun YJ, Lee JA, Nguyen SA, Rizk HG, Meyer TA, Lambert PR. Transcutaneous Electrical Nerve Stimulation for Treatment of Tinnitus: A Systematic Review and Meta-analysis. Otol Neurotol. Aug 2020;41(7):e767-e775. doi:10.1097/MAO.0000000000002712. https://www.ncbi.nlm.nih.gov/pubmed/32472915
- Zeng FG, Richardson M, Tran P, Lin H, Djalilian H. Tinnitus Treatment Using Noninvasive and Minimally Invasive Electric Stimulation: Experimental Design and Feasibility. Trends Hear. Jan-Dec 2019;23:2331216518821449. doi:10.1177/2331216518821449. https://www.ncbi.nlm.nih.gov/pubmed/30803416
- Riha C, Guntensperger D, Kleinjung T, Meyer M. Recovering Hidden Responder Groups in Individuals Receiving Neurofeedback for Tinnitus. Front Neurosci . 2022;16:867704. doi:10.3389/fnins.2022.867704. https://www.ncbi.nlm.nih.gov/pubmed/35812211
- Zarzycki MZ, Domitrz I. Stimulation-induced side effects after deep brain stimulation - a systematic review. Acta neuropsychiatrica. Apr 2020;32(2):57-64. doi:10.1017/neu.2019.35. https://www.ncbi.nlm.nih.gov/pubmed/31452489
- AANS. American Association of Neurological Surgeons. Deep Brain Stimulation. Availabel at https://www.aans.org/en/Patients/Neurosurgical-Conditions-and-Treatments/Deep-Brain-Stimulation Accessed 01/17/2023. 2023;
- Akkuzu B, Yilmaz I, Cakmak O, Ozluoglu LN. Efficacy of misoprostol in the treatment of tinnitus in patients with diabetes and/or hypertension. Auris Nasus Larynx . Sep 2004;31(3):226-32. doi:10.1016/j.anl.2004.03.005. https://www.aurisnasuslarynx.com/article/S0385-8146(04)00087-2/fulltext
- Briner W, House J, O'Leary M. Synthetic prostaglandin E1 misoprostol as a treatment for tinnitus. Arch Otolaryngol Head Neck Surg. Jun 1993;119(6):652-4. doi:10.1001/archotol.1993.01880180068013. https://jamanetwork.com/journals/jamaotolaryngology/article-abstract/621642
- Crinnion CL, McCart GM. Misoprostol for tinnitus. Ann Pharmacother. Jul-Aug 1995;29(7-8):782-4. doi:10.1177/106002809502907-823. https://journals.sagepub.com/doi/10.1177/106002809502907-823?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub 0pubmed
- Yilmaz I, Akkuzu B, Cakmak O, Ozlüoglu LN. Misoprostol in the treatment of tinnitus: a double-blind study. Otolaryngol Head Neck Surg. May 2004;130(5):604-10. doi:10.1016/j.otohns.2003.08.027. https://journals.sagepub.com/doi/10.1016/j.otohns.2003.08.027?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub 0pubmed
- Bayar N, Boke B, Turan E, Belgin E. Efficacy of amitriptyline in the treatment of subjective tinnitus. J Otolaryngol. Oct 2001;30(5):300-3. doi:10.2310/7070.2001.19597. https://www.ncbi.nlm.nih.gov/pubmed/11771024
- Sullivan M, Katon W, Russo J, Dobie R, Sakai C. A randomized trial of nortriptyline for severe chronic tinnitus. Effects on depression, disability, and tinnitus symptoms. Arch Intern Med. Oct 11 1993;153(19):2251-9. https://www.ncbi.nlm.nih.gov/pubmed/8215728
- Zoger S, Svedlund J, Holgers KM. The effects of sertraline on severe tinnitus suffering--a randomized, double-blind, placebo-controlled study. Journal of clinical psychopharmacology. Feb 2006;26(1):32-9. doi:10.1097/01.jcp.0000195111.86650.19. https://www.ncbi.nlm.nih.gov/pubmed/16415703
- Savage J, Waddell A. Tinnitus. BMJ clinical evidence. Oct 20 2014;2014 https://www.ncbi.nlm.nih.gov/pubmed/25328113
- Witkin JM, Lippa A, Smith JL, Cook JM, Cerne R. Can GABAkines quiet the noise? The GABA(A) receptor neurobiology and pharmacology of tinnitus. Biochem Pharmacol. Jul 2022;201:115067. doi:10.1016/j.bcp.2022.115067. https://www.ncbi.nlm.nih.gov/pubmed/35504315
- Jufas NE, Wood R. The use of benzodiazepines for tinnitus: systematic review. J Laryngol Otol. Jul 2015;129 Suppl 3:S14-22. doi:10.1017/S0022215115000808. https://www.ncbi.nlm.nih.gov/pubmed/25858126
- Tavares MP, Bahmad F, Jr. Analysis of Gabapentin's Efficacy in Tinnitus Treatment: A Systematic Review. Ann Otol Rhinol Laryngol. Mar 2022;131(3):303-311. doi:10.1177/00034894211018921. https://www.ncbi.nlm.nih.gov/pubmed/34036823
- Azevedo AA, Figueiredo RR. Tinnitus treatment with acamprosate: double-blind study. Braz J Otorhinolaryngol. Sep-Oct 2005;71(5):618-23. doi:10.1016/s1808-8694(15)31266-0. https://www.ncbi.nlm.nih.gov/pubmed/16612523
- Farhadi M, Salem MM, Asghari A, Daneshi A, Mirsalehi M, Mahmoudian S. Impact of Acamprosate on Chronic Tinnitus: A Randomized-Controlled Trial. Ann Otol Rhinol Laryngol. Nov 2020;129(11):1110-1119. doi:10.1177/0003489420930773. https://www.ncbi.nlm.nih.gov/pubmed/32500717
- Sharma DK, Kaur S, Singh J, Kaur I. Role of acamprosate in sensorineural tinnitus. Indian J Pharmacol. Jan 2012;44(1):93-6. doi:10.4103/0253-7613.91876. https://www.ncbi.nlm.nih.gov/pubmed/22345878
- Suckfull M, Althaus M, Ellers-Lenz B, et al. A randomized, double-blind, placebo-controlled clinical trial to evaluate the efficacy and safety of neramexane in patients with moderate to severe subjective tinnitus. BMC Ear Nose Throat Disord . Jan 11 2011;11:1. doi:10.1186/1472-6815-11-1. https://www.ncbi.nlm.nih.gov/pubmed/21223542
- Chung J, Lee DY, Kim JS, Kim YH. Effectiveness of Intratympanic Dexamethasone Injection for Tinnitus Treatment: A Systematic Review and Meta-Analysis. Clin Exp Otorhinolaryngol. Feb 2022;15(1):91-99. doi:10.21053/ceo.2021.01459. https://www.ncbi.nlm.nih.gov/pubmed/35144363
- de Cates C, Winters R. Intratympanic Steroid Injection. StatPearls . StatPearls Publishing Copyright © 2022, StatPearls Publishing LLC.; 2023.
- van Zon A, Smulders YE, Ramakers GG, et al. Effect of unilateral and simultaneous bilateral cochlear implantation on tinnitus: A Prospective Study. Laryngoscope. Apr 2016;126(4):956-61. doi:10.1002/lary.25493. https://www.ncbi.nlm.nih.gov/pubmed/26255618
- Amoodi HA, Mick PT, Shipp DB, Friesen LM, Nedzelski JM, Chen JM, Lin VY. The effects of unilateral cochlear implantation on the tinnitus handicap inventory and the influence on quality of life. Laryngoscope. Jul 2011;121(7):1536-40. doi:10.1002/lary.21851. https://www.ncbi.nlm.nih.gov/pubmed/21647911
- Poncet-Wallet C, Mamelle E, Godey B, et al. Prospective Multicentric Follow-up Study of Cochlear Implantation in Adults With Single-Sided Deafness: Tinnitus and Audiological Outcomes. Otol Neurotol. Apr 2020;41(4):458-466. doi:10.1097/MAO.0000000000002564. https://www.ncbi.nlm.nih.gov/pubmed/32176124
- Marinelli JP, Anzalone CL, Prummer CM, et al. Electrical stimulation of the cochlea for treatment of chronic disabling tinnitus: an open-label trial towards the development of an implantable device. J Transl Med. Jan 29 2022;20(1):56. doi:10.1186/s12967-022-03271-4. https://www.ncbi.nlm.nih.gov/pubmed/35093126
- He M, Li X, Liu Y, et al. Electroacupuncture for Tinnitus: A Systematic Review. PLoS One. 2016;11(3):e0150600. doi:10.1371/journal.pone.0150600. https://www.ncbi.nlm.nih.gov/pubmed/26938213
- Liu F, Han X, Li Y, Yu S. Acupuncture in the treatment of tinnitus: a systematic review and meta-analysis. Eur Arch Otorhinolaryngol. Feb 2016;273(2):285-94. doi:10.1007/s00405-014-3341-7. https://www.ncbi.nlm.nih.gov/pubmed/25344063
- Kim JI, Choi JY, Lee DH, Choi TY, Lee MS, Ernst E. Acupuncture for the treatment of tinnitus: a systematic review of randomized clinical trials. BMC Complement Altern Med. Jul 17 2012;12:97. doi:10.1186/1472-6882-12-97. https://www.ncbi.nlm.nih.gov/pubmed/22805113
- Spankovich C, Bishop C, Johnson MF, Elkins A, Su D, Lobarinas E, Le Prell CG. Relationship between dietary quality, tinnitus and hearing level: data from the national health and nutrition examination survey, 1999-2002. Int J Audiol . Oct 2017;56(10):716-722. doi:10.1080/14992027.2017.1331049. https://www.ncbi.nlm.nih.gov/pubmed/28553744
- Tang D, Tran Y, Shekhawat GS, Burlutsky G, Mitchell P, Gopinath B. Dietary Fibre Intake and the 10-Year Incidence of Tinnitus in Older Adults. Nutrients . Nov 17 2021;13(11)doi:10.3390/nu13114126.
- Jarach CM, Lugo A, Garavello W, et al. The Role of Diet in Tinnitus Onset: A Hospital-Based Case-Control Study from Italy. Nutrients. Jan 25 2023;15(3)doi:10.3390/nu15030621. https://mdpi-res.com/d_attachment/nutrients/nutrients-15-00621/article_deploy/nutrients-15-00621-v2.pdf?version=1675317249
- Chen S, Yang X, Jiang Y, et al. Associations Between Physical Activity, Tinnitus, and Tinnitus Severity. Ear Hear. May-Jun 01 2023;44(3):619-626. doi:10.1097/AUD.0000000000001306. https://www.ncbi.nlm.nih.gov/pubmed/36404413
- Aljuaid SM, Mirza AA, Habib LA, AlHarthi LA, Alansari BM, AlQahtani BG, Althobaiti YA. Does Caffeine Intake Increase the Incidence of Tinnitus? A Systematic Review. Int Arch Otorhinolaryngol. Oct 2021;25(4):e628-e632. doi:10.1055/s-0040-1718965. https://www.ncbi.nlm.nih.gov/pubmed/34737834
- Lee SY, Jung G, Jang MJ, Suh MW, Lee JH, Oh SH, Park MK. Association of Coffee Consumption with Hearing and Tinnitus Based on a National Population-Based Survey. Nutrients. Oct 4 2018;10(10)doi:10.3390/nu10101429.
- De Luca P, Cassandro C, Ralli M, et al. Dietary Restriction for The Treatment of Meniere's Disease. Translational medicine @ UniSa. May 2020;22:5-9. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7265917/pdf/tm-22-005.pdf
- Shim T, Strum DP, Mudry A, Monfared A. Hold the Salt: History of Salt Restriction as a First-line Therapy for Meniere's Disease. Otol Neurotol . Jul 2020;41(6):855-859. doi:10.1097/MAO.0000000000002635. https://www.ncbi.nlm.nih.gov/pubmed/32221112
- Webster KE, George B, Lee A, et al. Lifestyle and dietary interventions for Ménière's disease. Cochrane Database Syst Rev. Feb 27 2023;2(2):Cd015244. doi:10.1002/14651858.CD015244.pub2. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9969956/pdf/CD015244.pdf
- Hussain K, Murdin L, Schilder AG. Restriction of salt, caffeine and alcohol intake for the treatment of Meniere's disease or syndrome. Cochrane Database Syst Rev . Dec 31 2018;12(12):CD012173. doi:10.1002/14651858.CD012173.pub2. https://www.ncbi.nlm.nih.gov/pubmed/30596397 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6516805/pdf/CD012173.pdf
- Di Berardino F, Zanetti D. Delayed Immunomodulatory Effect of Cow Milk-Free Diet in Ménière's Disease. J Am Coll Nutr. Feb 2018;37(2):149-153. doi:10.1080/07315724.2017.1364181. https://air.unimi.it/bitstream/2434/559678/2/s1-ln2603257195844769-1939656818Hwf-1383107426IdV-46837038326032571PDF_HI0001.pdf
- Meijers SM, Lieftink AF, Stegeman I, Smit AL. Coping in Chronic Tinnitus Patients. Front Neurol. 2020;11:570989. doi:10.3389/fneur.2020.570989. https://www.ncbi.nlm.nih.gov/pubmed/33329312
- Beukes EW, Manchaiah V, Andersson G, Allen PM, Terlizzi PM, Baguley DM. Situationally influenced tinnitus coping strategies: a mixed methods approach. Disabil Rehabil. Dec 2018;40(24):2884-2894. doi:10.1080/09638288.2017.1362708. https://www.ncbi.nlm.nih.gov/pubmed/28793790
- Dauman N, Dauman R. An Empowerment Model for Individuals with Chronic Tinnitus. Ear Hear. Mar/Apr 2021;42(2):425-442. doi:10.1097/AUD.0000000000000946. https://www.ncbi.nlm.nih.gov/pubmed/32976248
- Fludra M, Kobosko J, Gos E, Paluchowska J, Skarzynski H. Ego-resiliency and Tinnitus Annoyance. J Am Acad Audiol. May 2022;33(5):270-276. doi:10.1055/a-1804-6601. https://www.ncbi.nlm.nih.gov/pubmed/35318619
- VA. US Department of Veterans Affairs: Progressive Tinnitus Management. available at https://www.research.va.gov/research_in_action/Progressive-Tinnitus-Management.cfm Published 08/01/2018. Accessed 01/24/2023. 2018;
- Edmonds CM, Clark KD, Thielman EJ, Henry JA. Progressive Tinnitus Management Level 3 Skills Education: A 10-Year Clinical Retrospective. Am J Audiol . Sep 2022;31(3):567-578. doi:10.1044/2022_AJA-22-00003. https://www.ncbi.nlm.nih.gov/pubmed/35973115
- Kutyba J, Jedrzejczak WW, Gos E, Bienkowska K, Raj-Koziak D, Skarzynski PH. Self-help interventions chosen by subjects with chronic tinnitus - a retrospective study of clinical patients. Int J Audiol . Aug 2022;61(8):686-691. doi:10.1080/14992027.2021.1964040. https://www.ncbi.nlm.nih.gov/pubmed/34410211
Wellness
Specialists
1-800-226-2370 - This service is FREE
7:30 AM - 12 AM (ET) Mon-Fri | 9 AM - 12 AM (ET) Sat-Sun