Life Extension Magazine®

As We See It: Why We Test Insulin Blood Levels
Excess insulin can hide a smoldering diabetic condition by temporarily suppressing glucose and A1c. If insulin blood levels are elevated, correctable actions can be taken before serious illnesses manifest.
By William Faloon.

Customers who order our blood test panels often ask why we measure fasting insulin.
One reason is that higher fasting insulin levels are correlated with lower life expectancy1 and increased risks of cancer 2-5 and cardiovascular disorders.6-8
Insulin production is regulated by blood sugar levels and hormones. Fasting insulin increases in response to insulin resistance.9,10
At first, higher insulin levels can initially help drive glucose out of the blood into cells.10
As insulin resistance worsens, even greater insulin secretion fails to adequately normalize blood glucose.10
A missed opportunity for early diagnosis occurs when fasting insulin is omitted from blood panels that measure glucose and A1c.
Higher levels of insulin can temporarily reduce glucose and A1c in a way that masks glycemic control issues.10

In other words, glucose and A1c may appear “normal” on blood test results. But without testing fasting insulin, this may create a false sense of security by not recognizing that the “excess” insulin is helping to keep glucose and A1c within acceptable ranges.11
Before full-blown type II diabetes manifests, suboptimal glycemic control is associated with increasing risks of the most common diseases12 of aging.13-16
Further, worsening glycemic control can silently contribute to diabetes, leading to peripheral nerve damage (neuropathy), chronic kidney disease, and/or loss of vision (retinopathy).17
Newly diagnosed diabetics often ask why so many morbidities afflict them so quickly. The answer is these pathologies were festering for years as a result of suboptimal metabolic control, which could have been identified earlier with proper blood tests.
Some studies have shown that fasting insulin levels are a more accurate predictor of cardiometabolic risk, compared to tests for insulin resistance.18,19
One of the most serious global health problems today is metabolic disorders related to obesity and insulin resistance.20,21 Effective methods (diet and exercise) can slow or halt progression to type II diabetes—but prevention is critical.
That’s why it’s essential to include fasting insulin with glucose and A1c blood testing to get a more accurate understanding of your glycemic status.
Type II diabetes is surging higher worldwide among all age groups.
The Centers for Disease Control and Prevention is running public service ads (one copied on this page) warning that one in three American adults is at risk for prediabetes.20
The term “prediabetes” can be misleading. Few realize that the initial stages of glucose imbalance inflict severe tissue damage. This happens before full-blown type II diabetes is officially diagnosed.16
These pathologies are not limited to adults. There was an astounding 95% increase in Americans under age 20 living with type II diabetes between 2001-2017.22
Need for Early Intervention

Most cases of type II diabetes begin when cells slowly become resistant to insulin.20
When this occurs, glucose buildup in blood causes the pancreas to secrete higher levels of insulin to force glucose into cells. This temporarily helps compensate for insulin resistance in target tissues (e.g., skeletal, muscle, liver).
During the period of insulin resistance, weight gain may be an outward sign of loss of glycemic control. This happens as elevated levels of glucose + insulin contribute to unwanted fat storage.1,23
Weight gain and physical inactivity increase the risk of developing insulin resistance.20
As insulin resistance worsens, insulin levels often rise as the pancreas attempts to compensate and literally force glucose into target tissues that have become resistant to the action of insulin at a cellular level.1
If a blood test reveals high fasting insulin before glucose and A1c become elevated, this provides an opportunity to identify diabetes earlier in the process, before extensive damage occurs.
Published data suggest elevated fasting insulin can be a useful diagnostic tool for identifying early-stage insulin resistance.24
One study found insulin resistance to be the most important predictive risk factor in the development of coronary artery disease.25
Other studies recognize the prognostic value of fasting insulin and suggest that hyperinsulinemia (high fasting insulin) is often both a result and a driver of insulin resistance. 16
A consistent association exists between hypertension (high blood pressure) and elevated insulin. 26
Mechanistic factors have been identified to explain why tissue damage associated with “excess” insulin and insulin resistance causes blood pressure to spike.27
Kidney Damage

Chronic kidney disease is surging, coinciding with an increased prevalence of obesity, hypertension, and diabetes.
Insulin resistance and hypertension predispose to premature atherosclerosis28,29 and other pathologies that contribute to chronic kidney disease.21,32
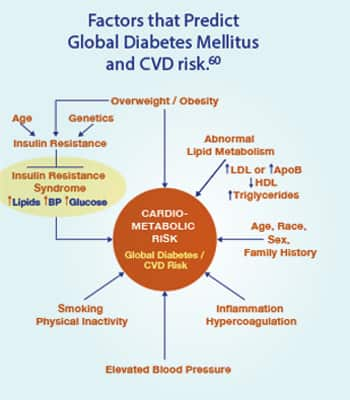
Cardiometabolic syndrome, (a constellation of metabolic dysfunction characterized by insulin resistance, impaired glucose tolerance, dyslipidemia, hypertension, and intra-abdominal obesity) is associated with an increase in cardiovascular disease33,34 and kidney failure.35,36
Recognition of the role of insulin resistance and hyperinsulinemia in cardiometabolic syndrome provides a rationale to measure fasting insulin blood levels.
Based on the currently available data, we believe that fasting insulin above 5 μIU/mL is likely suboptimal. Steps that can be taken to improve metabolic health include a healthy, plant-based diet low in simple sugar, processed animal products, and saturated fat, and high in nutrients that help support metabolic health.37
Physical activity is also important for metabolic health.
Along with these lifestyle changes, and if appropriate for an individual based upon his/ her unique health needs, the use of medications under a physician’s care, including metformin38,39 and/or an SGLT2 inhibitor40,41 like Jardiance® can further improve metabolic health before full-blown type II diabetes manifests.
Advanced-stage kidney disease is currently irreversible. Identifying causative risk factors early with blood tests that include fasting insulin can enable one to take corrective actions in time.
What you need to know
Hyperinsulinemia and Cancer
A massive review article (369 references) published in 2021 describes the health risks and mechanistic dangers of excess insulin.46
What follows is an excerpt from this review titled: “Hyperinsulinemia in Obesity, Inflammation and Cancer”:
“Hyperinsulinemia was associated with a 2-fold risk of cancer death.47 This increase of cancer mortality is also observed in people with normal body weight if they had hyperinsulinemia.48 Therefore, hyperinsulinemia is associated with increased risk of both cancer incidence and death. However, unlike hyperglycemia, there is no widely accepted insulin concentration to define hyperinsulinemia, so it is difficult to compare across studies. Nevertheless, the rationale to study the contribution of hyperinsulinemia to cancer is strong.”
Cancer
Insulin has direct and indirect effects on cancer cell progression, proliferation, and metastasis.42,43
Studies investigating the association between hyperinsulinemia and cancer-related mortality have been inconsistent. Reasons might include the upper-limit reference range used to define hyperinsulinemia.
For example, the standard reference range for fasting insulin begins at 2.6 uIU/mL and extends to a startling high of 24.9 uIU/mL.44
Life Extension® long ago urged readers to target fasting insulin below 7.0 uIU/mL with optimalfasting insulin below 5.0 uIU/mL.
Today’s laboratory reference ranges don’t define hyperinsulinemia until fasting insulin rises above 24.9 uIU/mL. This is 3-to-5-times higher than what we consider optimal.
A study found lung cancer incidence doubled in men in the highest quartile of fasting insulin compared to those in the lowest insulin quartile. The conclusions from this study were:
“Higher fasting serum insulin concentrations, as well as the presence of insulin resistance, appear to be associated with an elevated risk of lung cancer.” 45
A gender-based subgroup analysis of seven different studies found significant association between fasting insulin and cancer mortality. The risk of cancer mortality in men with high insulin levels is almost double as compared to those having lower fasting insulin levels.42
Ignorance regarding “optimal” fasting insulin levels might be obscuring the impact of high, but “normal” insulin resistance markers on cancer risk and overall cancer mortality.
Why the controversy?
Life Extension® has published articles over the decades about the disease risks associated with excess fasting insulin.
Yet there are inconsistencies in the literature and in medical opinion as to what levels of fasting insulin increase disease risks.
One impediment in reaching consensus is varying definitions.
Hyperinsulinemia is sometimes defined as:46
“The amount of insulin in blood being higher than considered normal.”
With laboratory reference ranges defining “normal” as high as 24.9 uIU/mL, doctors who test fasting insulin may not realize the risks in patients with higher than optimal insulin levels.
We believe fasting insulin levels above 5.0-7.0 uIU/mL may indicate cellular insulin resistance, yet today’s laboratory reference ranges define normal as between 2.6 and 24.9 uIU/mL.
A better definition of hyperinsulinemia is a condition in which:
“There are excess levels of insulin circulating in the blood relative to glucose.”
Even this definition can make interpretation of blood test results challenging since the majority of Americans today are overweight and prone to large fluctuations in fasting glucose and insulin levels.
Even thin people can suffer from insulin resistance, which is another reason for testing blood for fasting insulin.
A mass education program about insulin resistance is urgently needed, along with knowledge that it can be detectedearly by properly interpreting fasting insulin, glucose and A1c blood test results.
Cellular Insulin Resistance
The cells of many people with impaired glycemic control tend to be more resistant to insulin-stimulated glucose uptake than those with normal glucose tolerance.
The ability of insulin to stimulate cellular glucose uptake varies widely among individuals.
Resistance to insulin-stimulated glucose uptake and compensatory hyperinsulin-emia represents a basic defect in many patients in the early stage of type II diabetes.1
As the condition worsens, insulin-producing pancreatic cells fail, thus some type II diabetics to require insulin injections.1
Increases in pancreatic insulin production can temporarily prevent elevations of glucose and A1c. This does not mean that this compensatory (hyperinsulinemic) response is benign.
Early-stage diabetic development (and related complications) is predictable by including fasting insulin with conventional blood test panels.
What you can do today!

Insulin resistance can be reversed by aggressive dietary and lifestyle changes, including increases in physical activity.40,49-54
Nutrients with glucose-lowering effects can help in combination with diet and more physical activity. For some this is not enough, and for these individuals, medications like metformin and/or an SGLT2 inhibitor may also be needed to optimize metabolic health. SGLT2 inhibitors are sold under brand names that include Jardiance®, forxiga®, Invokana® and others.
An AMPK-activating drug called metformin improves insulin sensitivity and can reduce fasting insulin levels indirectly, largely as a result of improvement in peripheral insulin sensitivity at the cellular level.49,55
Sodium-Glucose Co-Transporter 2 inhibitor (SGLT2 inhibitor) drugs increase urinary excretion of glucose from blood. This drug class helps reduce the progression of chronic kidney disease in patients with type II diabetes and reduces adverse cardiovascular outcomes in many of these patients.56
Some studies show SGLT2 inhibitors reduce fasting insulin, likely a result of the reduction of excess blood glucose.57-59
The first step, however, is blood tests that measureglucose, A1c and fasting insulin.
We suggest you target:
- Fasting Glucose between 80-86 mg/dL
- Hemoglobin A1c between 5.0%-5.4%
- Fasting Insulin < 5 μIU/mL
While these numbers are not achievable by everyone, you can at least lower them to safer ranges by initiating steps to improve glycemic status.
A popular blood test panel outlined on the next page includes A1c, glucose, fasting insulin, lipids, C-reactive protein, and other measures.
Commercial labs charge about $2,000 for these tests, but once a year we discount the popular Male and Female Panels down to $224.
You can order these tests 24 hours/day by calling 1-800-208-3444 or visting www.LifeExtenson.com/bloodtests
I hope this editorial explains why fasting insulin is included in many of our comprehensive blood test panels.
The article on page 24 of this issue describes an easy-to-take fiber approved by the FDA in 2020. One of the benefits found with this soluble plant fiber is reduced glucose and insulin blood levels.
For longer life,
William Faloon
References
- Kolb H, Kempf K, Röhling M, et al. Insulin: too much of a good thing is bad. BMC Medicine. 20202020/08/21;18(1):224.
- Gallagher EJ, LeRoith D. Hyperinsulinaemia in cancer. Nat Rev Cancer. 2020Nov;20(11):629-44.
- Dugnani E, Balzano G, Pasquale V, et al. Insulin resistance is associated with the aggressiveness of pancreatic ductal carcinoma. Acta Diabetol. 2016Dec;53(6):945-56.
- Sun W, Lu J, Wu S, et al. Association of insulin resistance with breast, ovarian, endometrial and cervical cancers in non-diabetic women. Am J Cancer Res. 2016;6(10):2334-44.
- Loftfield E, Freedman ND, Lai GY, et al. Higher Glucose and Insulin Levels Are Associated with Risk of Liver Cancer and Chronic Liver Disease Mortality among Men without a History of Diabetes. Cancer Prev Res (Phila). 2016Nov;9(11):866-74.
- de Rooij SR, Dekker JM, Kozakova M, et al. Fasting insulin has a stronger association with an adverse cardiometabolic risk profile than insulin resistance: the RISC study. Eur J Endocrinol. 2009 Aug;161(2):223-30.
- Zhang X, Li J, Zheng S, et al. Fasting insulin, insulin resistance, and risk of cardiovascular or all-cause mortality in non-diabetic adults: a meta-analysis. Biosci Rep. 2017Oct 31;37(5).
- Ormazabal V, Nair S, Elfeky O, et al. Association between insulin resistance and the development of cardiovascular disease. Cardiovasc Diabetol. 2018Aug 31;17(1):122.
- Gutch M, Kumar S, Razi SM, et al. Assessment of insulin sensitivity/resistance. Indian J Endocrinol Metab. 2015 Jan-Feb;19(1):160-4.
- Available at: https://www.uptodate.com/contents/clinical-presentation-diagnosis-and-initial-evaluation-of-diabetes-mellitus-in-adults?search=hb%20A1c%20test&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1. Accessed March, 8, 023.
- Thomas DD, Corkey BE, Istfan NW, et al. Hyperinsulinemia: An Early Indicator of Metabolic Dysfunction. Journal of the Endocrine Society. 2019;3(9):1727-47.
- McLarty RP, Alloyce JP, Chitema GG, et al. Glycemic control, associated factors, acute complications of Type 1 Diabetes Mellitus in children, adolescents and young adults in Tanzania. Endocrinology, Diabetes & Metabolism. 2021;4(2):e00200.
- Ali MK, Bullard KM, Saydah S, et al. Cardiovascular and renal burdens of prediabetes in the USA: analysis of data from serial cross-sectional surveys, 1988-2014. Lancet Diabetes Endocrinol. 2018 May;6(5):392-403.
- Park C, Guallar E, Linton JA, et al. Fasting glucose level and the risk of incident atherosclerotic cardiovascular diseases. Diabetes Care. 2013Jul;36(7):1988-93.
- Brutsaert EF, Shitole S, Biggs ML, et al. Relations of Postload and Fasting Glucose With Incident Cardiovascular Disease and Mortality Late in Life: The Cardiovascular Health Study. J Gerontol A Biol Sci Med Sci. 2016Mar;71(3):370-7.
- Giri B, Dey S, Das T, et al. Chronic hyperglycemia mediated physiological alteration and metabolic distortion leads to organ dysfunction, infection, cancer progression and other pathophysiological consequences: An update on glucose toxicity. Biomedicine & Pharmacotherapy. 2018 2018/11/01/;107:306-28.
- Available at: https://www.cdc.gov/diabetes/managing/problems.html#:~:text=Common%20diabetes%20health%20complications%20include,how%20to%20improve%20overall%20health. Accessed March 9, 2023, 2023.
- Röhling M, Kempf K, Kolb H, et al. The Epidemiological Boehringer Ingelheim Employee Study (Part 3): Association of Elevated Fasting Insulin Levels but Not HOMA-IR With Increased Intima Media Thickness and Arteriosclerosis in Middle-Aged Persons. Front Cardiovasc Med. 2021;8:752789.
- de Rooij SR, Dekker JM, Kozakova M, et al. Fasting insulin has a stronger association with an adverse cardiometabolic risk profile than insulin resistance: the RISC study. Eur J Endocrinol. 2009 Aug;161(2):223-30.
- Available at: https://www.cdc.gov/diabetes/basics/insulin-resistance.html. Accessed March, 9, 2023.
- Ahmed B, Sultana R, Greene MW. Adipose tissue and insulin resistance in obese. Biomedicine & Pharmacotherapy. 2021 2021/05/01/;137:111315.
- Available at: https://www.cdc.gov/media/releases/2021/p0824-youth-diabetes.html. Accessed March, 7, 2023.
- Faruque S, Tong J, Lacmanovic V, et al. The Dose Makes the Poison: Sugar and Obesity in the United States - a Review. Pol J Food Nutr Sci. 2019;69(3):219-33.
- ter Horst KW, Gilijamse PW, Koopman KE, et al. Insulin resistance in obesity can be reliably identified from fasting plasma insulin. Int J Obes (Lond). 2015Dec;39(12):1703-9.
- Adeva-Andany MM, Martinez-Rodriguez J, Gonzalez-Lucan M, et al. Insulin resistance is a cardiovascular risk factor in humans. Diabetes Metab Syndr. 2019Mar-Apr;13(2):1449-55.
- Park SK, Jung JY, Choi WJ, et al. Elevated fasting serum insulin level predicts future development of hypertension. Int J Cardiol. 2014 Mar 15;172(2):450-5.
- Zhou MS, Wang A, Yu H. Link between insulin resistance and hypertension: What is the evidence from evolutionary biology? Diabetol Metab Syndr. 2014Jan 31;6(1):12.
- Reaven GM, Knowles JW, Leonard D, et al. Relationship between simple markers of insulin resistance and coronary artery calcification. J Clin Lipidol. 2017Jul-Aug;11(4):1007-12.
- Fakhrzadeh H, Sharifi F, Alizadeh M, et al. Relationship between insulin resistance and subclinical atherosclerosis in individuals with and without type 2 diabetes mellitus. J Diabetes Metab Disord. 2015;15:41.
- Janus A, Szahidewicz-Krupska E, Mazur G, et al. Insulin Resistance and Endothelial Dysfunction Constitute a Common Therapeutic Target in Cardiometabolic Disorders. Mediators Inflamm. 2016 2016/06/20;2016:3634948.
- Westergren HU, Svedlund S, Momo RA, et al. Insulin resistance, endothelial function, angiogenic factors and clinical outcome in non-diabetic patients with chest pain without myocardial perfusion defects. Cardiovasc Diabetol. 2016Feb 19;15(1):36.
- da Silva AA, do Carmo JM, Li X, et al. Role of Hyperinsulinemia and Insulin Resistance in Hypertension: Metabolic Syndrome Revisited. Can J Cardiol. 2020May;36(5):671-82.
- Bornfeldt KE, Tabas I. Insulin resistance, hyperglycemia, and atherosclerosis. Cell Metab. 2011Nov 2;14(5):575-85.
- Kirk EP, Klein S. Pathogenesis and pathophysiology of the cardiometabolic syndrome. J Clin Hypertens (Greenwich). 2009 Dec;11(12):761-5.
- Oishi Y, Manabe I. Organ System Crosstalk in Cardiometabolic Disease in the Age of Multimorbidity. Front Cardiovasc Med. 2020;7:64.
- Yerram P, Karuparthi PR, Saab G, et al. The cardiometabolic syndrome and chronic kidney disease. Current Cardiovascular Risk Reports. 2008 2008/03/01;2(2):95-100.
- Castro-Barquero S, Ruiz-León AM, Sierra-Pérez M, et al. Dietary Strategies for Metabolic Syndrome: A Comprehensive Review. Nutrients. 2020 Sep 29;12(10).
- Lv Z, Guo Y. Metformin and Its Benefits for Various Diseases. Front Endocrinol (Lausanne). 2020;11:191.
- Szymczak-Pajor I, Wenclewska S, Śliwińska A. Metabolic Action of Metformin. Pharmaceuticals (Basel). 2022Jun 30;15(7).
- Ni L, Yuan C, Chen G, et al. SGLT2i: beyond the glucose-lowering effect. Cardiovasc Diabetol. 2020Jun 26;19(1):98.
- Xu B, Li S, Kang B, et al. The current role of sodium-glucose cotransporter 2 inhibitors in type 2 diabetes mellitus management. Cardiovasc Diabetol. 2022May 25;21(1):83.
- Ghanavati M, Rahmani J, Rinaldi G, et al. Fasting Insulin and Risk of Cancer Related Mortality in Non-diabetic Adults: A Dose-response Meta-analysis of Cohort Studies. Curr Diabetes Rev. 2020;16(4):357-63.
- Goodwin PJ, Ennis M, Bahl M, et al. High insulin levels in newly diagnosed breast cancer patients reflect underlying insulin resistance and are associated with components of the insulin resistance syndrome. Breast Cancer Res Treat. 2009Apr;114(3):517-25.
- Available at: https://www.labcorp.com/tests/004333/insulin. Accessed March 9, 2023.
- Argirion I, Weinstein SJ, Mannisto S, et al. Serum Insulin, Glucose, Indices of Insulin Resistance, and Risk of Lung Cancer. Cancer Epidemiol Biomarkers Prev. 2017 Oct;26(10):1519-24.
- Zhang AMY, Wellberg EA, Kopp JL, et al. Hyperinsulinemia in Obesity, Inflammation, and Cancer. Diabetes Metab J. 2021 May;45(3):285-311.
- Walraven I, van ‘t Riet E, Stehouwer CD, et al. Fasting proinsulin levels are significantly associated with 20 year cancer mortality rates. The Hoorn Study. Diabetologia. 2013May;56(5):1148-54.
- Tsujimoto T, Kajio H, Sugiyama T. Association between hyperinsulinemia and increased risk of cancer death in nonobese and obese people: A population-based observational study. Int J Cancer. 2017 Jul 1;141(1):102-11.
- Diabetes Prevention Program Research G. Long-term effects of lifestyle intervention or metformin on diabetes development and microvascular complications over 15-year follow-up: the Diabetes Prevention Program Outcomes Study. Lancet Diabetes Endocrinol. 2015 Nov;3(11):866-75.
- Ethan M. Balk M, MPH, Amy Earley, BS, Gowri Raman, MD, MS, Esther A. Avendano, BA, Anastassios G. Pittas, MD, MS, and Patrick L. Remington, MD, MPH Combined Diet and Physical Activity Promotion Programs to Prevent Type 2 Diabetes Among Persons at Increased Risk: A Systematic Review for the Community Preventive Services Task Force. Annals of Internal Medicine. 2015;163(6):437-51.
- Munir KM, Chandrasekaran S, Gao F, et al. Mechanisms for food polyphenols to ameliorate insulin resistance and endothelial dysfunction: therapeutic implications for diabetes and its cardiovascular complications. Am J Physiol Endocrinol Metab. 2013Sep 15;305(6):E679-86.
- Mirabelli M, Chiefari E, Arcidiacono B, et al. Mediterranean Diet Nutrients to Turn the Tide against Insulin Resistance and Related Diseases. Nutrients. 2020Apr 12;12(4).
- Yaribeygi H, Atkin SL, Simental-Mendia LE, et al. Molecular mechanisms by which aerobic exercise induces insulin sensitivity. J Cell Physiol. 2019Aug;234(8):12385-92.
- Hawley JA, Lessard SJ. Exercise training-induced improvements in insulin action. Acta Physiol (Oxf). 2008Jan;192(1):127-35.
- Herman R, Kravos NA, Jensterle M, et al. Metformin and Insulin Resistance: A Review of the Underlying Mechanisms behind Changes in GLUT4-Mediated Glucose Transport. Int J Mol Sci. 2022Jan 23;23(3).
- Mima A. Sodium-Glucose Cotransporter 2 Inhibitors in Patients with Non-Diabetic Chronic Kidney Disease. Adv Ther. 2021 May;38(5):2201-12.
- Tobe K, Suganami H, Kaku K. Sodium-glucose cotransporter 2 inhibitor, tofogliflozin, shows better improvements of blood glucose and insulin secretion in patients with high insulin levels at baseline. J Diabetes Investig. 2018Jul;9(4):862-9.
- Okura T, Fujioka Y, Nakamura R, et al. The sodium-glucose cotransporter 2 inhibitor ipragliflozin improves liver function and insulin resistance in Japanese patients with type 2 diabetes. Sci Rep. 2022Feb 3;12(1):1896.
- Esterline RL, Vaag A, Oscarsson J, et al. MECHANISMS IN ENDOCRINOLOGY: SGLT2 inhibitors: clinical benefits by restoration of normal diurnal metabolism? Eur J Endocrinol. 2018Apr;178(4):R113-R25.
- Kahn R. Metabolic Syndrome. Circulation. 2007;115(13):1806-11.
Wellness
Specialists
1-800-226-2370 - This service is FREE
7:30 AM - 12 AM (ET) Mon-Fri | 9 AM - 12 AM (ET) Sat-Sun