Life Extension Magazine®

Atherosclerosis in Sweden: Implications for Americans
A study found that 42% of Swedish study subjects without known heart disease had detectable atherosclerosis. Americans have even greater vascular risks. Low-cost blood tests can detect risk factors for atherosclerosis before major cardiovascular events strike.
By William Faloon.

The American Heart Association published a report on a study that detected atherosclerosis in 42% of Swedish study subjects without known heart disease.1
Compared to Americans, most Swedish citizens have lower vascular risks.2
In 2019, the percentage of obese people in Sweden was 13.1% compared to 40% in the United States.3
Coronary heart disease deaths are 22.5% higher in the United States than in Sweden.4
These data about artery disease in Sweden likely indicate greater atherosclerosis prevalence in the United States.

Autopsy studies on young Americans consistently show evidence of atherosclerosis.5,6
Recognized risk factors of severe artery disease include hypertension,7-9 elevated lipids7,10-12 diabetes, 7,13 and/or obesity.7,14
A common misconception is that atherosclerosis is a modern-day phenomenon.
Studies using high-resolution images of mummified bodies from different world regions reveal the opposite. Atherosclerosis has plagued mankind for thousands of years.15
Atherosclerosis is the term used to describe damage and obstruction that occurs in the linings of our arteries.16
When arterial blood flow is impeded or blocked, the result can be death or disability from a stroke or heart attack.16
A misconception about atherosclerosis is that it did not exist in prior historic eras. I've heard so-called experts claim that people didn't suffer coronary artery disease in the past because their diets were so "natural.""
These "experts" do not have sufficient data and have no basis to claim that atherosclerosis is a recent phenomenon. All they can cite is that few people developed heart disease in the past compared to today.
The reason more people weren't having heart attacks back then is that most died before the age of 40-60 from diseases that are now curable.
The advantage we have today is being able to delay atherosclerotic progression and reduce our risk of coronary heart attack and ischemic stroke.
Atherosclerosis in Ancient Cultures
A study published in 2011 found definitive or probable atherosclerosis present in mummified bodies that lived during every era of ancient Egypt studied.17
In 2013, The Lancet showed that mummified humans dating back 4,000 years and spanning several geographic locations/cultures all suffered from clogged arteries.15
According to the lead investigator of The Lancet study:
"The fact that we found similar levels of atherosclerosis in all of the different cultures we studied, all of whom had very different lifestyles and diets, suggests that atherosclerosis may have been far more common in the ancient world than previously thought."15 —Randall Thompson, MD
Modern Era Atherosclerosis
A 2021 Swedish study found a1.8-times greater prevalence of atherosclerosis in people aged 60-64 compared to those 50-54 years old.1
As we at Life Extension have long argued, atherosclerosis is a disease of aging that has long been prevalent.18
It took modern computed tomography imaging to document probable signs of heart disease in 34% of mummified humans whose estimated mean age at death was 43 years. Those who died at an estimated mean age of 32 years were less likely to show signs of atherosclerosis.15
These findings suggest that arterial disease has always been widespread. The encouraging news is that methods to prevent and even reverse it have been validated in modern clinical studies.
What Caused Atherosclerosis In The Mummified Bodies?

In seeking to identify what caused atherosclerosis in the mummified bodies, The Lancet researchers speculated that it could have been the high levels of inflammation these primitive people were exposed to from constant infections and a non-hygienic environment.15
People with severe inflammatory conditions (like rheumatoid arthritis 19,20 and lupus21,22) suffer accelerated atherosclerosis.
Multiple studies of modern people link chronic inflammation as an independent risk factor for stroke22 and heart attack.22-24
One study investigated a large group of older individuals who were followed for 17 years. Those with the highest levels of inflammatory blood markers were over three-times more likely to suffer sudden cardiac death compared to people with the lowest levels.25
It's comforting to live in an era where chronic inflammation can be identified with blood tests and corrective actions taken to suppress elevated inflammatory markers.
Why Is Atherosclerosis So Common?
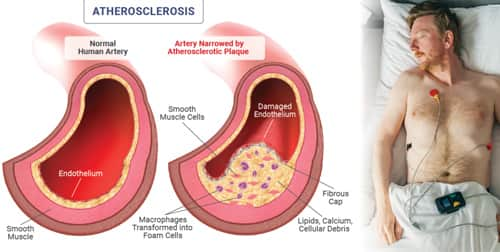
We know that multiple factors can alter arterial function and damage the delicate arterial lining (endothelium). These negative factors include excess dietary intake of the wrong kinds of fats,26 sugars,27 high salt intake,28 and tobacco smoke. 29,30
Most of us are born with an intact endothelium that lines our arteries and protects against the formation of atherosclerosis.
As we age, our arterial lining endures chronic insult from internal and external factors that results in endothelial damage leading to atherosclerosis. Progressing blockage of blood vessels results in decreased blood flow to the heart, kidneys, and brain.18,31
Health issues linked to atherosclerosis are a leading reason why most aging people die in the United States.16
Those who understand the many causes of atherosclerosis should not be surprised that it is so common. What's appalling is the number of people who continue to succumb to atherosclerotic diseases because of apathy and ignorance.
What Can You Do About It?
Endothelial dysfunction is one reason why atherosclerosis is such a common worldwide pathology.31
As the inner arterial wall (the endothelium) becomes dysfunctional, it enables atherosclerotic lesions to initiate, progress, and eventually occlude blood flow. 31
As you will read on page 40 of this issue, a combination of low-cost nutrients has been shown to help modulate endothelial dysfunction and improve blood flow.
Annual Blood Test Sale

We at Life Extension® have long encouraged annual blood tests to screen for underlying arterial disease and take corrective actions when risk factors like homocysteine, C-reactive protein, and LDL are at dangerous levels.
Once a year, prices are discounted so our supporters can assess their status and initiate preemptive measures before illnesses strike.
On page 11 there is a description of the popular Male and Female Blood Test panels.
Commercial labs charge thousands for these tests, but readers of this publication obtain them for only $224 during the Blood Test Super Sale.
To order the Male or Female Blood Test Panel at these low prices, call 1-800-208-3444 (24 hours) or visit: www.LifeExtension.com/sales/lab-tests
For longer life,
William Faloon
References
- Bergstrom G, Persson M, Adiels M, et al. Prevalence of Subclinical Coronary Artery Atherosclerosis in the General Population. Circulation. 2021 Sep 21;144(12):916-29.
- Eriksson M, Holmgren L, Janlert U, et al. Large improvements in major cardiovascular risk factors in the population of northern Sweden: the MONICA study 1986-2009. J Intern Med. 2011 Feb;269(2):219-31.
- Available at: https://www.commonwealthfund.org/publications/issue-briefs/2020/jan/us-health-care-global-perspective-2019. Accessed February, 22, 2023.
- Available at: https://www.worldlifeexpectancy.com/cause-of-death/coronary-heart-disease/by-country/. Accessed February, 20, 2023.
- Webber BJ, Seguin PG, Burnett DG, et al. Prevalence of and risk factors for autopsy-determined atherosclerosis among US service members, 2001-2011. JAMA. 2012 Dec 26;308(24):2577-83.
- Gongora-Rivera F, Labreuche J, Jaramillo A, et al. Autopsy prevalence of coronary atherosclerosis in patients with fatal stroke. Stroke. 2007 Apr;38(4):1203-10.
- Malakar AK, Choudhury D, Halder B, et al. A review on coronary artery disease, its risk factors, and therapeutics. J Cell Physiol. 2019 Aug;234(10):16812-23.
- Allen NB, Siddique J, Wilkins JT, et al. Blood pressure trajectories in early adulthood and subclinical atherosclerosis in middle age. JAMA. 2014 Feb 5;311(5):490-7.
- Poznyak AV, Sadykhov NK, Kartuesov AG, et al. Hypertension as a risk factor for atherosclerosis: Cardiovascular risk assessment. Front Cardiovasc Med. 2022;9:959285.
- Abd Alamir M, Goyfman M, Chaus A, et al. The Correlation of Dyslipidemia with the Extent of Coronary Artery Disease in the Multiethnic Study of Atherosclerosis. J Lipids. 2018;2018:5607349.
- Gidding SS, Allen NB. Cholesterol and Atherosclerotic Cardiovascular Disease: A Lifelong Problem. J Am Heart Assoc. 2019 Jun 4;8(11):e012924.
- Hoogeveen RC, Gaubatz JW, Sun W, et al. Small dense low-density lipoprotein-cholesterol concentrations predict risk for coronary heart disease: the Atherosclerosis Risk In Communities (ARIC) study. Arterioscler Thromb Vasc Biol. 2014 May;34(5):1069-77.
- Poznyak AV, Litvinova L, Poggio P, et al. Effect of Glucose Levels on Cardiovascular Risk. Cells. 2022 Sep 28;11(19).
- Available at: https://www.cdc.gov/obesity/data/adult.html#:~:text=Obesity%20is%20a%20common%2C%20serious,42.4%25%20in%202017%20%E2%80%93%202018. Accessed February, 20, 2023.
- Thompson RC, Allam AH, Lombardi GP, et al. Atherosclerosis across 4000 years of human history: the Horus study of four ancient populations. Lancet. 2013 Apr 6;381(9873):1211-22.
- Available at: https://www.nhlbi.nih.gov/health/atherosclerosis. Accessed February, 20, 2023.
- Allam AH, Thompson RC, Wann LS, et al. Atherosclerosis in ancient Egyptian mummies: the Horus study. JACC Cardiovasc Imaging. 2011 Apr;4(4):315-27.
- Head T, Daunert S, Goldschmidt-Clermont PJ. The Aging Risk and Atherosclerosis: A Fresh Look at Arterial Homeostasis. Front Genet. 2017;8:216.
- Szekanecz Z, Kerekes G, Der H, et al. Accelerated atherosclerosis in rheumatoid arthritis. Ann N Y Acad Sci. 2007 Jun;1108:349-58.
- Tanasescu C, Jurcut C, Jurcut R, et al. Vascular disease in rheumatoid arthritis: from subclinical lesions to cardiovascular risk. Eur J Intern Med. 2009 Jul;20(4):348-54.
- Roman MJ, Shanker BA, Davis A, et al. Prevalence and correlates of accelerated atherosclerosis in systemic lupus erythematosus. N Engl J Med. 2003 Dec 18;349(25):2399-406.
- Parikh NS, Merkler AE, Iadecola C. Inflammation, Autoimmunity, Infection, and Stroke: Epidemiology and Lessons From Therapeutic Intervention. Stroke. 2020 Mar;51(3):711-8.
- Marnane M, Merwick A, Sheehan OC, et al. Carotid plaque inflammation on 18F-fluorodeoxyglucose positron emission tomography predicts early stroke recurrence. Ann Neurol. 2012 May;71(5): 709-18.
- Available at: https://www.heart.org/en/health-topics/consumer-healthcare/what-is-cardiovascular-disease/inflammation-and-heart-disease. Accessed February, 22, 2023.
- Hussein AA, Gottdiener JS, Bartz TM, et al. Inflammation and sudden cardiac death in a community-based population of older adults: the Cardiovascular Health Study. Heart Rhythm. 2013 Oct;10(10):1425-32.
- Sacks FM, Lichtenstein AH, Wu JHY, et al. Dietary Fats and Cardiovascular Disease: A Presidential Advisory From the American Heart Association. Circulation. 2017 Jul 18;136(3):e1-e23.
- Loader J, Meziat C, Watts R, et al. Effects of Sugar-Sweetened Beverage Consumption on Microvascular and Macrovascular Function in a Healthy Population. Arterioscler Thromb Vasc Biol. 2017 Jun;37(6):1250-60.
- Dickinson KM, Clifton PM, Keogh JB. Endothelial function is impaired after a high-salt meal in healthy subjects. Am J Clin Nutr. 2011 Mar;93(3):500-5.
- Hahad O, Arnold N, Prochaska JH, et al. Cigarette Smoking Is Related to Endothelial Dysfunction of Resistance, but Not Conduit Arteries in the General Population-Results From the Gutenberg Health Study. Front Cardiovasc Med. 2021;8:674622.
- Messner B, Bernhard D. Smoking and cardiovascular disease: mechanisms of endothelial dysfunction and early atherogenesis. Arterioscler Thromb Vasc Biol. 2014 Mar;34(3):509-15.
- Gimbrone MA, Jr., Garcia-Cardena G. Endothelial Cell Dysfunction and the Pathobiology of Atherosclerosis. Circ Res. 2016 Feb 19;118(4):620-36.
Wellness
Specialists
1-800-226-2370 - This service is FREE
7:30 AM - 12 AM (ET) Mon-Fri | 9 AM - 12 AM (ET) Sat-Sun