Life Extension Magazine®

What’s Missing from Most Multivitamins
Millions of Americans take a multivitamin, including 68% of seniors. Yet many older adults have inadequate intake of essential nutrients.
Scientifically reviewed by: Dr. Gary Gonzalez, MD, in October 2024. Written by: Michael Downey.
Millions of Americans take a multivitamin, including 68% of seniors.1
Yet surveys going back decades show that many older adults have inadequate intake of essential micronutrients.2
Major reasons for this are aging people who take no supplement or those who rely on a multivitamin with low potencies or inactive forms of specific nutrients.
Deficiencies Are Common with Age
Most Americans don’t get enough of the nutrients they need.
There are a variety of reasons.
Many older people eat less, making them more prone to develop vitamin and mineral deficiencies.
Chronic conditions increase the need for some vitamins and minerals.
Medications may lower levels of critical nutrients, especially B vitamins. And older adults have a decreased capacity to absorb and use many nutrients.2
Fortunately, most readers of this magazine supplement with optimal potencies and forms of vitamins, minerals, and plant extracts.
Deficient Multivitamins!
Most multivitamins don’t fix the problem of vitamin and mineral deficiencies. Rather, they give many people a false sense of security that they’re getting all the nutrients they need.
The vast majority of multivitamins use nutritional targets set by the federal government. These targets tend to represent the minimum level of any nutrient required to sustain life, not the amount that will maximize healthy longevity.
In addition, few available products contain optimal forms of nutrients.
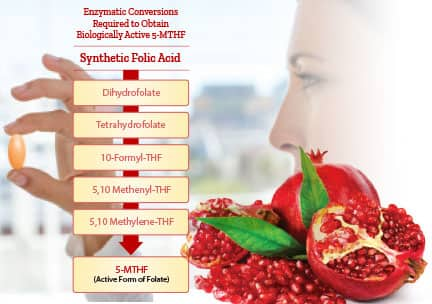
For example, folic acid (or folate) needs to be converted by the body into the metabolically active form, 5-MTHF.
This is of particular importance, as approximately 40% of people carry a gene variant that impairs their ability to convert folate into its active form: 5-methyltetrahydrofolate (5-MTHF).8
Huge Nutritional Gaps
Despite most older Americans now taking a multinutrient formula, many have insufficient levels of important nutrients.
A survey by the National Institutes of Health published in 2017 found that 14% of so-called “full-spectrum, multivitamin-multimineral supplement” users were still deficient in at least one nutrient.3
Deficiency is defined as a nutrient level being so low that it causes a specific disease to manifest. In the case of vitamin D, a bone-wasting disease called rickets develops in response to very low vitamin D.
Insufficiency describes less-than-optimal levels of an essential nutrient.
A study of American hospitalized patients found nearly 40% were deficient in vitamin D, defined as 25-hydroxvitamin D blood levels less than 20 ng/mL.4
To put this 40% who were deficient into context, much of conventional medicine still fails to recognize what minimal level of vitamin D is needed to avoid health problems.
Researchers debate whether frank deficiency should be defined as 25-hydroxyvitamin D blood levels less than 20 ng/mL or 12 ng/mL.5 Either level is frighteningly low based on data published in recent decades.
For example, the preponderance of evidence clearly shows that one should strive for 25-hydroxyvitamin D blood levels above 30 ng/mL. Life Extension® has advocated that 50-80 ng/mL of 25-hydroxyvitamin D is likely ideal.
When looking at data where 30 ng/mL of 25-hydroxyvitamin D is defined as the low point before a person enters a disease risk category, an astounding 69% of Americans are below this minimal (30 ng/mL) vitamin D blood marker, including some taking popular multivitamin supplements.6,7
Micronutrient Intake in the U.S.
Using data from the National Health and Nutrition Examination Survey (NHANES) 2007-2010, researchers from the Council for Responsible Nutrition determined that large proportions of the population have intakes below the estimated average requirements (EAR).
Below are some of the percentages of Americans (ages four and over) who fail to meet the estimated average requirement:9
| Nutrient | Percent Under Average |
| Vitamin A | 35 % |
| Vitamin C | 31 % |
| Vitamin D | 74% |
| Vitamin E | 67% |
| Calcium | 39% |
| Magnesium | 46% |
“Average requirement” does not consider people with underlying health issues whose need for certain nutrients can be strikingly high.10
There is an urgent need for more Americans to ensure at least adequate intake of nutrients that were identified decades ago as essential for better health and well-being.
Building a Better Multivitamin

To effectively promote health, aging individuals often need to take higher potencies of certain nutrients.
To meet the vitamin and mineral needs of older people, scientists created a formula designed to deliver the optimal potencies and forms of critical nutrients.
Compared to a popular multivitamin made by a pharmaceutical company, this formula has long provided:
- 2 times the magnesium,
- 2 times the zinc,
- 2 times the vitamin D,
- 2.5 times the vitamin B3,
- 3 times the vitamin E,
- 8 times the vitamin C,
- 10 times the selenium,
- 10 times the biotin,
- 12 times the vitamin B12,
- 25 times the vitamin B6, and
- 50 times the vitamin B1.
What you need to know
An Ideal Multivitamin
- Older adults stand to benefit from a multivitamin, but studies show that they frequently have nutrient deficiencies.
- Leading multivitamins omit nutrients, provide insufficient amounts, and fail to use the optimal forms of some nutrients.
- Scientists have designed a blend of vitamins, minerals, and plant-based nutrients that delivers the broadest array of health-promoting compounds in optimal potencies and forms.
- Taking a better vitamin and mineral blend can significantly improve overall health and shorten the length of illnesses.
Nutrients in Optimal Forms
In addition to higher potencies, it’s vital to get a wide range of nutrients in optimal forms. This includes nutrients not generally found in multivitamins, such as:
- The mineral boron,
- Mixed tocopherols (forms of vitamin E), each with demonstrated biological benefits,
- The antioxidant alpha-lipoic acid, and
- Plant extracts, such as the bioflavonoid apigenin and the carotenoid lycopene.
And optimal forms of nutrients should be consumed, including a highly stable chromium and the meta- bolically active form of folate, 5-MTHF.
Key Nutrients
Here’s a look at a few nutrients that most Americans should look for in a multivitamin:
Vitamin D
Vitamin D is best known for supporting bone health. It also promotes healthy cell division, immune function, and more.11,12 Multivitamin formulas’ potencies used to be an abysmally low 400-800 IU, even in recent years. Minimum vitamin D levels to achieve what most consider “sufficient” potency should deliver 2,000 IU of vitamin D daily.
Some people take an additional 1,000-5,000 IU of vitamin D3 daily to achieve optimal blood levels.
Vitamin C
Vitamin C is associated with immune health, likely due to its ability to stimulate the production and function of immune cells.13,14 It is also vital to the formation of collagen, the connective tissue found throughout healthy arterial walls, skin, bones, and teeth.13 A superior formula should provide far more than the meager 60-90 mg found in most commercial multivitamin formulas.
B Vitamins
B vitamins help to release the energy stored in nutrients that the body’s cells need to carry out their daily functions.15 The various B vitamins work together to maintain overall health. That is why an ideal vitamin contains readily metabolized forms of riboflavin (B2), vitamin B12, vitamin B6, folate, and others.
Mixed Vitamin E Tocopherols
The four forms of vitamin E tocopherols—alpha, beta, delta, and gamma—work together to optimize health. For example, evidence indicates that combining alpha and gamma tocopherols is better for helping to reduce chronic inflammation and oxidative stress than taking either nutrient alone.16 All four forms should be taken daily. Many commercial multivitamins contain only synthetic alpha tocopherol and none of the other natural forms of vitamin E.
Alpha-Lipoic Acid
Alpha-lipoic acid is a natural compound that helps to protect vitamin C and glutathione so that they can fight against damaging free radicals.17-19 Most multi-vitamins don’t contain it.
Selenium
The mineral selenium promotes heart and brain health, supports healthy inflammatory and immune responses.20,21 What most people don’t realize is that selenium comes in different forms, each having distinct beneficial properties. These “forms” include: high- selenium yeast, Se-methyl L-selenocysteine, and sodium selenite. Each has specific beneficial properties.
Molybdenum
Most multivitamins don’t contain sufficient potencies of molybdenum. This mineral is required for several enzymatic activities, including those that detoxify alcohol and metabolize sulfur.22
Vitamin A
Vitamin A is best obtained from two separate sources: the fatty acid retinyl acetate and the pigment beta-carotene. This essential vitamin promotes vision, immune health, free-radical defenses, formation of thyroid hormones, healthy skin and mucous membranes, and the growth of bone, teeth, and soft tissues. Its use has been associated with decreased risk of certain skin cancers.23
Taking a daily multinutrient formula that includes optimal forms and meaningful potencies can provide powerful health benefits.
Optimal Form of Folate
Folate must be converted in the body by a complex series of enzymatic steps before it can be used.
But 5-MTHF (5-methyltetrahydrofolate) is a form of folate that is already metabolically active and can be used by tissues immediately. This specific form was shown in one study to be seven times more bioavailable than folic acid.24
This is critical for those with certain genetic enzyme defects that make folate metabolism less efficient.25
Summary
Many Americans can benefit from a multivitamin.
Research shows that micronutrient deficiencies are common.
Many leading multivitamin brands contain inadequate nutrient potencies, and do not contain the optimal forms.
Taking a daily formula with a broad array of health-promoting vitamins, minerals, and plant extracts may benefit overall health.
If you have any questions on the scientific content of this article, please call a Life Extension® Wellness Specialist at 1-866-864-3027.
References
- Available at: https://news.gallup.com/poll/166541/half-americans-vitamins-regularly.aspx. Accessed October 2, 2018.
- Available at: https://www.ncbi.nlm.nih.gov/books/NBK51837/. Accessed October 16, 2020.
- Bird JK, Murphy RA, Ciappio ED, et al. Risk of Deficiency in Multiple Concurrent Micronutrients in Children and Adults in the United States. Nutrients. 2017 Jun 24;9(7):655.
- Parva NR, Tadepalli S, Singh P, et al. Prevalence of Vitamin D Deficiency and Associated Risk Factors in the US Population (2011-2012). Cureus. 2018 Jun 5;10(6):e2741.
- Available at: https://www.medicinenet.com/vitamin_d_deficiency/article.htm. Accessed October 25, 2020.
- Available at: /magazine/2010/1/startling-findings-about-vitamin-d-levels-in-life-extension-members. Accessed October 25, 2020.
- Chowdhury R, Kunutsor S, Vitezova A, et al. Vitamin D and risk of cause specific death: systematic review and meta-analysis of observational cohort and randomised intervention studies. BMJ. 2014 Apr 1;348:g1903.
- Moll S, Varga EA. Homocysteine and MTHFR Mutations. Circulation. 2015 Jul 7;132(1):e6-9.
- Wallace TC, McBurney M, Fulgoni VL, 3rd. Multivitamin/mineral supplement contribution to micronutrient intakes in the United States, 2007-2010. J Am Coll Nutr. 2014;33(2):94-102.
- Dwyer J. Dietary Requirements of Adults. In: Caballero B, ed. Encyclopedia of Food Sciences and Nutrition. Oxford: Academic Press; 2003:1863-8.
- Christakos S, Hewison M, Gardner DG, et al. Vitamin D: beyond bone. Ann N Y Acad Sci. 2013 May;1287:45-58.
- Wang H, Chen W, Li D, et al. Vitamin D and Chronic Diseases. Aging Dis. 2017 May;8(3):346-53.
- Data on file.
- Lykkesfeldt J, Michels AJ, Frei B. Vitamin C. Adv Nutr. 2014 Jan 1;5(1):16-8.
- Available at: https://www.ncbi.nlm.nih.gov/books/NBK538510/. Accessed October 16, 2020.
- Devaraj S, Leonard S, Traber MG, et al. Gamma-tocopherol supplementation alone and in combination with alpha-tocopherol alters biomarkers of oxidative stress and inflammation in subjects with metabolic syndrome. Free Radic Biol Med. 2008 Mar 15;44(6):1203-8.
- Bustamante J, Lodge JK, Marcocci L, et al. Alpha-lipoic acid in liver metabolism and disease. Free Radic Biol Med. 1998 Apr;24(6):1023-39.
- Data on file.
- Tibullo D, Li Volti G, Giallongo C, et al. Biochemical and clinical relevance of alpha lipoic acid: antioxidant and anti-inflammatory activity, molecular pathways and therapeutic potential. Inflamm Res. 2017 Nov;66(11):947-59.
- Data on file.
- Solovyev ND. Importance of selenium and selenoprotein for brain function: From antioxidant protection to neuronal signalling. J Inorg Biochem. 2015 Dec;153:1-12.
- Data on file.
- Kim J, Park MK, Li WQ, et al. Association of Vitamin A Intake With Cutaneous Squamous Cell Carcinoma Risk in the United States. JAMA Dermatol. 2019 Jul 31;155(11):1260-8.
- Willems FF, Boers GH, Blom HJ, et al. Pharmacokinetic study on the utilisation of 5-methyltetrahydrofolate and folic acid in patients with coronary artery disease. Br J Pharmacol. 2004 Mar;141(5):825-30.
- Shelton RC, Sloan Manning J, Barrentine LW, et al. Assessing Effects of l-Methylfolate in Depression Management: Results of a Real-World Patient Experience Trial. Prim Care Companion CNS Disord. 2013;15(4).
Wellness
Specialists
1-800-226-2370 - This service is FREE
7:30 AM - 12 AM (ET) Mon-Fri | 9 AM - 12 AM (ET) Sat-Sun