Life Extension Magazine®

PET Scans: Understanding The Nature Of Cancer
Cancer patients and their doctors now have access to a superior imaging technology in PET scans. Dr. Richard Black seeks to establish a standardized system for accurate interpretation of PET scans, thereby saving lives.
Scientifically reviewed by: Dr. Shaylind Benson, ND, in October 2024. Written by: Kirk Stokel.
| PREAMABLE
The purpose of this article is to enlighten oncologists about superior imaging methodologies that can enable them to better recommend treatment options to their patients. It is very technical and most readers will find it challenging to comprehend. This article is meant for those stricken with cancer and their team of oncology experts. It is not for general audiences. By Kirk Stokel When cancer strikes, timely, accurate information is of the essence. Time, because the sooner an accurate diagnosis is made, the greater the chances of stopping the disease before it’s too late. Information, because cancer is a living thing that constantly changes both itself and its environment. It’s vital to know not only where a cancer has taken hold, but also what it is doing: how rapidly is it growing, is it spreading, is it destroying or invading adjacent tissue? Physicians have been able to learn at least basic information about a cancer’s physical location since the invention of medical X-rays in the late 19th century.1-3 Today’s CT (computerized tomography) and MRI (magnetic resonance imaging) scanners provide exquisite details about the size, shape, and other anatomical features of an abnormal mass. Other techniques, however, are needed to determine if the mass is indeed a cancer, and if so, how aggressively it is spreading and invading.3
Until recently, that functional information that relates to the metabolic activities of cells could be obtained only by invasive means such as biopsies or open surgeries. Much of that is changing now, with the advent of so-called functional imaging studies that can tell an experienced expert a great deal about an unknown mass. In the right hands, such information can allow an expert to distinguish between a malignant cancer and a benign mass, scar tissue, or focus of infection. Positron Emission Tomography, or PET scanning, is rapidly emerging as one of the most useful forms of diagnostic imaging, especially with regard to diagnosing and managing cancer. 4-6 Like all imaging studies, however, PET scans are fraught with pitfalls for the uninitiated. As PET scanners appear in more and more hospitals, there’s a growing need for standardization of interpretation and reporting of results. Above all, there’s a need for experienced physicians to read the scans and provide useful information to the physicians who order them. Sadly, that level of rigor and expertise is lacking in many hospitals around the country, according to Dr. Richard Black, Director of Nuclear Medicine and PET Imaging for Radisphere National Radiology Group based in Cleveland, Ohio. We caught up with Dr. Black recently to get a better understanding of PET scanning in general, and specifically to provide readers with a clear idea of the pitfalls, as well as the strengths, presented by this powerful new technology. Let’s start with a basic synopsis of what a PET scanner does, and how it obtains functional or metabolic information about a tumor or other suspicious mass. Then we’ll see real patients from Dr. Black’s casebook on how PET scans are being used in caring for patients with malignancies. We’ll touch briefly on the practical limitations of PET scan technology. Then we’ll focus on Dr. Black’s breakthrough efforts to change the way PET scans are interpreted and reported. Dr. Black is leading the field in developing standardized, reproducible reports on literally tens of thousands of patients for his customers that are situated throughout the United States and abroad and thus allowing oncologists and other clinicians to derive maximum benefit from these imaging studies. What Is PET Scanning?
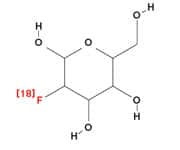
PET scanners produce functional information about a suspected tumor through the use of a technique that differs entirely from conventional radiology studies. The essence of the modus operandi—the method of operation—of PET is based in the world of quantum physics. To conduct a PET scan, a technician injects a patient with a radioactive tracer material. The most commonly used material is fluorodeoxyglucose, or FDG. (See figure 1.) FDG consists of a molecule of glucose chemically linked to a radioisotope of fluorine called 18F. Like glucose, FDG is taken up into cells through a variety of specialized transporters and enzyme systems. The more metabolically active a cell is, the more glucose, and hence, FDG, it takes up.7 Cancer cells are highly metabolically active because of their rapid rate of reproduction; that means that they take up FDG much more avidly than surrounding normal tissue.8-10 The radioactive fluorine isotope in FDG is constantly emitting a stream of positrons, the antimatter equivalent of electrons. Each time a positron encounters an electron, the two particles annihilate each other in a matter-antimatter implosion, giving off a pair of photons (little packets of energy).11 The photons trigger a signal on detectors built into the PET scanner (See figure 2), and powerful computers assemble all of those signals into a coherent 3-dimensional image. Areas of the most intense glucose utilization, then, will “light up” as areas of high metabolic activity, which indicate the presence of cancer with a very high likelihood.7,9,11-13 Of course, there’s a trade-off for everything. While they produce vivid images of cells’ functional, metabolic activity, PET scans by themselves don’t produce a very precise anatomical picture. The solution is to combine the findings of a PET scan with those of a conventional imaging study (usually a CT scan) that can provide detailed anatomical information. With both PET and CT images “in register,” they can be readily superimposed to provide the diagnostician with both anatomical and metabolic information about the tissues and organs of interest. This is the PET/CT scan that is in use today.
How Are PET/CT Scans Used?With their rich supply of functional data on cellular metabolism, PET scans have tremendous potential in oncology. Dr. Black points out that, “A PET scan report should tell a clinician what he or she really wants and needs to know to facilitate and optimize individual patient management. The report should not be a long, convoluted listing of findings without interpretation and explanation. Most importantly, a PET scan should be able to change and assist how a clinician manages a patient.” According to Dr. Black, PET scans can correctly and successfully change patient management in an average of 30% of cases compared to conventional imaging techniques that include CT, MRI, plain film radiography etc. Other experts estimate that figure as high as 38%.14 These findings translate to a huge impact on outcomes, given the millions of cases of cancer in the US each year.15 FDG PET/CT scans are useful for differentiating benign from malignant lesions, evaluating tumor stage, monitoring the response to therapy and detecting tumor recurrence in a variety of malignancies.5 Here are a few case studies from Dr. Black’s files and the medical literature, indicating just how PET scans were used, and the impact they had on management.
Case #1: Assigning a higher stage to a known cancer.13 A 63-year-old man with a recent diagnosis of a primary colon cancer was evaluated by PET/CT scan following surgical removal of the tumor. At surgery, no spread to lymph nodes, and no tumor metastases were found. The PET/CT study, however, revealed metastases in the patient’s liver, resulting in a higher clinical stage. Because of this finding, the treatment options for this patient were dramatically changed.
Case #2: Assigning a lower stage to a known cancer.13 An 85-year-old man with a recent diagnosis of Merkel cell carcinoma, a rare and highly aggressive skin cancer, had undergone a CT scan that suggested three separate metastases in the liver. A PET/CT scan was done to confirm that metastatic spread, but instead it showed completely normal liver tissue. This patient’s disease was “down-staged,” and he was spared unnecessary chemotherapy.
Case #3: Monitoring a patient’s favorable response to therapy.13,16 A 79-year-old woman with a history of lung cancer, treated with chemotherapy in April of 2009, underwent a PET/CT scan in July of that year. A CT scan still showed a nodule at the site of the original cancer, and was read as showing persistent disease. The PET scan, however, revealed a complete metabolic response to treatment, indicating in fact no residual tumor.
Case #4: Monitoring a patient’s unfavorable response to therapy.13 A 72-year-old woman with lung cancer, treated in November of 2010, was given a CT scan in February 2011 to determine her response. Her tumor had not changed size, and the scan was therefore interpreted as showing stable disease with no progression. A PET/CT scan that same day was more informative, demonstrating that in fact her left lung was highly metabolically active, indicating progressive disease. This patient required additional treatment.
In each of these cases, PET/CT studies provided valuable information about the metabolic activity of tissue. Such information that could not be obtained from the anatomic data provided by CT alone (or, in Case 3, by direct examination during surgery). These cases provide persuasive evidence that PET/CT scans change patient management in a variety of important ways. Let’s now examine some of the limitations of PET technology, and learn how Dr. Black is working to overcome these limitations to obtain the most useful information possible. |








Limitations of PET ScansAs with all medical testing, PET/CT scan interpretation is associated with one of two kinds of statistical errors. They can result in a “false negative” result, incorrectly indicating absence of a tumor, when in fact a tumor is present. False negatives can occur when factors are present that limit how much FDG a tumor can take up from the blood.13 This may happen with blood vessel narrowing that reduces blood flow to the tumor, or when a tumor has grown so fast that many of its cells die off. Other contributing factors may include the unique cellular characteristics of the individual tumor. On the other hand, a “false positive” i.e., incorrectly indicating presence of malignant tissue when cancer is absent, can arise when non-malignant cells have increased glucose uptake or utilization. This may occur in certain infections and with many inflammatory processes. False positive readings are not uncommon following cancer surgery, when a patient has residual inflammatory tissue that is incorrectly read as persistence of tumor. This can be circumvented with additional acquisitions of the abnormal area on the PET study and a proper understanding of the biochemistry of malignant and non-malignant conditions. But there’s another type of error that is of serious concern to Dr. Black. It has nothing to do with the technology, and everything to do with how the PET/CT study is being interpreted, which in and of itself can produce either false negative or false positive results. The rapid expansion of PET technology has resulted in a large number of studies being read by physicians who simply haven’t been adequately trained. The issue is compounded by a lack of standardization in the way scans are read. Surprisingly, many PET/CT reports are simply narratives, which are lacking in standard categories and in quantifiable numerical values. Furthermore, many inexperienced readers fail to routinely correct the quantitative degree of uptake in the area of abnormality that is detected by the scanner. The uptake defined on the scan will vary considerably depending upon the elapsed time from when the radiotracer was injected into the patient. There are other issues as well, including the patient’s body weight and the proper calibration of the PET scanner itself.17 Without addressing such issues, Black comments, it is nearly impossible to accurately monitor response to therapy, or to determine real progression of disease, and these are two of PET scanning’s most potentially valuable contributions. Even simply detecting a real tumor is much more difficult without a standardized, corrected reading. Since PET/CT scans do expose patients to radiation, Dr. Black believes that every scan should yield the maximum amount of information. “Too often,” he says, “Physicians reading these scans describe findings without insight or provision of clinically useful and applicable information.” Often times the reports are essentially a discourse on the anatomic findings obtained from the CT portion of the study with little emphasis placed on the information delineated on the PET component of the examination. In the space remaining, we’ll demonstrate how Dr. Black approaches the interpretation of PET scans with an eye towards providing that insight in a way that helps physicians, and ultimately patients, optimally manage the challenges of cancer care.
Standardized, Quantified PET/CT Scan Readings Provide Insight
Dr. Black optimizes his reading of PET/CT scans using five key features. This approach assures the oncologist that he is receiving the same kind and quality of information on every scan. That information can then be used to reliably monitor a patient’s response, or lack of response, to therapy. “In other words,” says Black, “the referring physician can compare apples with apples.” Here is a brief overview of Black’s 5 key report features, and why they are so vital: 1. PET/CT scan reporting should be quantitative. Too often reports contain only descriptive, qualitative information. Dr. Black showed one such report, in which the reader’s diagnosis was, “Hypermetabolic right upper lobe pulmonary mass.” Translated, that simply means that something in the lung was using glucose more rapidly than the rest of the body. There was no interpretation! Was the mass likely to be a tumor or not? There’s also no way to compare this kind of a reading with past or future scans, since no objective information is provided. Dr. Black reports a “standardized uptake value,” or SUV, on every object of concern in a scan.8,18 An SUV of greater than 2.5 is generally considered abnormal, providing a useful cut-off point for determining if an area is likely to be malignant or not. The numerical SUV also provides a value that can be compared with earlier or subsequent scans, an important improvement. The peer reviewed medical literature provides direction for the implementation and utilization of the SUV for different clinical situations and locations. 2. PET/CT reports should be reproducible, allowing different experts using different equipment to obtain similar results. “I’ve seen one lesion reported with an SUV of 10 from one facility, but only 5 at another on the same patient,” says Black. “That kind of information is virtually meaningless. I realized early on that, reading studies from a variety of different vendors and platforms that variability in the quantitative degree of uptake could be standardized to the liver parenchyma which should be a relatively consistent number from case to case and machine to machine. The process is simple by selecting an area of preserved normal, homogenous tissue in the liver, and using it to generate a corrected SUV for every area of concern that I read,” Dr. Black said. Black demonstrated his point with a scan that showed an uncorrected SUV of 10.4 in a case of suspected lung cancer recurrence — clearly an abnormal finding. Black’s correction factor, using an area of healthy liver, brought that SUV down to 2.0, a normal value. This patient might have undergone dangerous and unnecessary chemotherapy had the correction not been applied. This kind of correction has been recommended by major nuclear medicine experts.17 This approach is especially important and relevant when assessing the impact of therapeutic intervention whether it be systemic cytotoxic therapy (chemotherapy) or radiation therapy. By standardizing the numbers from one study to the next, the information now administered to the clinician is accurate, reproducible and can be used to predict response, stability or progression with a significantly greater degree of accuracy then anatomic imaging studies like CT and MRI. Astoundingly, Dr. Black has yet to see this approach implemented throughout the United States on review of thousands of FDG PET/CT studies undertaken nationwide. 3. PET/CT reports should focus on selected index lesions. There may be one or two, or five or ten “hotspots” indicating tumor activity generally grouped by anatomic localization.17 These lesions must be monitored from one study to the next in order to ascertain if the patient is responding to treatment. In cancer medicine, the patient’s prognosis is dependent on whether the treatment results in a complete disappearance of all pathological lesions (complete remission) or 50% or more reduction in these same lesions (partial remission). Again, this strategy allows each subsequent report to be compared with the original, enabling rapid and accurate measurement of changes over time or in response to therapy. The quantitative parameters uniquely applicable to PET imaging allow for more precise assessment of the clinical response to treatment, as metabolic changes (reflected in the degree of glucose uptake) on the PET scan change much earlier than do the anatomic abnormalities defined with CT or MRI. 4. PET scan reports should mandate comparative readings. That is, they should make reference to size, SUV, and other features of an index lesion(s) from previous scans, and they should explicitly point out increases or decreases and what they mean. This often means the radiologist needs to know if the patient has had prior studies, and if so, where they were done. It also obligates the current radiologist to request those studies for a side-by-side comparison with the current study. Of course it is also imperative that any imaging study be done before a therapeutic intervention (surgery, radiation, chemotherapy, immunotherapy, metabolic therapy, cryosurgery, high intensity focused ultrasound, etc). “Once treatment has been started,” said Black, “I have no way to tell if an area is getting worse or getting better without a baseline for comparison.” 5. Finally, PET scan reports should include image snapshots of the index lesions so that the ordering physician visualizes the areas of abnormality, rather than trying to create a mind picture based solely on a written report. You would think that these features would be more or less obvious requirements for any imaging technique whose purpose is to detect and track tissue abnormalities, be they cancer or any other pathology. Incredibly, Dr. Black was able to demonstrate dozens of reports containing none of the 5 key points above. “When I see a report like that,” Black says, “I feel terrible that the patient went through the whole scanning process without getting any useful information out of it.” Every one of Dr. Black’s reports contains a table with headings for anatomical information (location and size of the tumor), for functional information (the corrected SUV, and, most importantly one for his interpretation, including comparison with previous studies, and a likely explanation for abnormal findings. Black’s reports include statements such as “interim metabolic progression” (bad news, indicating that a tumor is more metabolically active than before), or “quantitative partial metabolic response” (good news, indicating that a tumor is at least partially responding to treatment). Any oncologist reading such a report immediately has a concise summary of the patient’s status at the time of the scan, a comparison with prior scans, and a clear understanding of what has changed and why. Thus the patient’s status is optimally presented to the clinician and an appropriate strategy can follow.
SummaryA diagnosis of cancer produces tremendous fear and uncertainty in patients and their loved ones. We need to trust that diagnostic studies aimed at understanding a cancer patient’s status do not add to the uncertainty, and don’t introduce more risk than necessary. PET/CT scanning offers a remarkably accurate and comprehensive way to look at patients being evaluated for a suspected cancer as well as pertaining to the followup of patients with known cancer as they progress or respond to therapy. But PET/CT scan interpretation is a mixture of genuine art and application of objective science, fraught with a variety of subjective pitfalls that can misdirect an inexpert reader to dangerously false conclusions. Dr. Richard Black is a tireless activist in the field of nuclear medicine, constantly exhorting his colleagues to better understand the technology involved in PET scans, to interpret them in a rigorous, standardized, and reproducible fashion, and to provide information that oncologists can immediately apply towards improving the care of their patients. The take home lessons of this article are summarized in the sidebar "What You Need to Know: Role of Functional PET Scans in Cancer Care." Commentary on "Understanding the Functional Nature of Cancer: The Value of PET (position emission tomography)"by Stephen B. Strum, MD, FACP, (Board-Certified Medical Oncologist) & Life Extension Scientific Advisory Board Member
All of us are patients at some time in our lives. Indeed, our life—and its quality—as well as our death—and its nature—is so evidently related to whether the healthcare delivered to us is wonderful, average, suboptimal or downright dangerous. In cancer medicine or oncology, the testing that is done to establish either the presence of cancer, to determine cancer extent (stage of disease), and to discern if the treatment we are receiving is working or not, are all crucial determinants of our outcome. But for this physician involved in cancer medicine for a half century, it is obvious that metaphorically speaking, healthcare itself is a sick patient with a dire prognosis. Many of you have heard me stress the importance of the key concept that “Status Begets Strategy.” I have chanted this theme in papers I have authored, in the book The Primer on Prostate Cancer by Strum & Pogliano, as well as in many lectures to patients and physicians. Status is what’s going on—what is the biologic reality of the patient as determined by every sense that we have available to us? Thus status relates to the patient’s history, the physical examination, laboratory testing, pathology evaluation and radiologic imaging. But blatantly lacking in today’s “healthcare” is standardization in reporting, and this deficiency spans virtually all of these areas of information relating to status. How can anyone intelligently direct our care when we do not know what’s going on, what is our baseline, and are we getting better or worse? How can medical doctors vary so wildly, yes wildly, in their reporting that one report can be a work of a truly dedicated physician and another report on the same issue be akin to a cartoon? What we have here is a horrendous problem in communication. It is Cool Hand Luke, MD, but what’s at stake is your life, and mine.
I have been frustrated for decades with the lack of a scientific approach in all realms of the medical record. In this article on PET (Positron Emission Tomography), the rational, logical and yes, standardized approach by Dr. Rick Black, a radiologist specializing solely in PET imaging is beautifully presented. Hallelujah! This is the way medical reports should be generated, whether they relate to imaging studies like PET, or to other radiology studies like TRUSP (transrectal ultrasound of the prostate), MRI of the prostate, bone scans, or CT studies, etc. This same scientific thinking should apply to how MDs report their physical examination findings, how the pathologist reports the results of biopsies or other surgical specimens, and even how laboratories report their findings (see Appendix F in The Primer on Prostate Cancer for examples of some of these objectified reports). The 5 key features of a solid medical report provided by Dr. Black should be foundational for every STATUS report involving a living entity i.e., you and me and everyone we know. How can we achieve what Dr. Black so elegantly presented? It won’t come from the physicians, since the lion’s share of healthcare practitioners are more comfortable with the status quo than with change. The only way to evolve medical reporting will come from patients and patient groups who are sufficiently empowered to voice their opinion—loudly and clearly—to those that have the power to effect a change—our elected officials. Remember, for the vast majority of us, it is we the people that are paying for our healthcare, and like my grandma from Poland once said, “When you ain’t got your health, you ain’t got nothing.” If you have any questions on the scientific content of this article, please call a Life Extension® Health Advisor at 1-866-864-3027. | |||||||||||
| References | |||||||||||
| 1. Freybott A. 100 years roentgen rays--a discovery conquers the medical world. Radiologe. 1995 Nov;35(11):866-70. 2. Macovski A. MRI: a charmed past and an exciting future. J Magn Reson Imaging. 2009 Nov;30(5):919-23. 3. Reed AB. The history of radiation use in medicine. J Vasc Surg. 2011 Jan;53(1 Suppl):3S-5S. 4. Warning K, Hildebrandt MG, Kristensen B, Ewertz M. Utility of 18FDG-PET/CT in breast cancer diagnostics—a systematic review. Dan Med Bull. 2011 Jul;58(7):A4289. 5. Yoon KT, Kim JK, Kim do Y, et al. Role of 18F-fluorodeoxyglucose positron emission tomography in detecting extrahepatic metastasis in pretreatment staging of hepatocellular carcinoma. Oncology. 2007;72 Suppl 1:104-10. 6. Gould MK, Maclean CC, Kuschner WG, Rydzak CE, Owens DK. Accuracy of positron emission tomography for diagnosis of pulmonary nodules and mass lesions: a meta-analysis. JAMA. 2001 Feb 21;285(7):914-24. 7. Avril N, Menzel M, Dose J, et al. Glucose metabolism of breast cancer assessed by 18F-FDG PET: histologic and immuno-histochemical tissue analysis. J Nucl Med. 2001 Jan;42(1):9-16. 8. Huang SC. Anatomy of SUV. Standardized uptake value. Nucl Med Biol. 2000 Oct;27(7):643-6. 9. Bustamante E, Pedersen PL. High aerobic glycolysis of rat hepatoma cells in culture: role of mitochondrial hexokinase. Proc Natl Acad Sci U S A. 1977 Sep;74(9):3735-9. 10. Lopez-Lazaro M. The Warburg effect: why and how do cancer cells activate glycolysis in the presence of oxygen? Anticancer Agents Med Chem. 2008 Apr;8(3):305-12. 11. Andresen GB, Ashkezari MD, Baquero-Ruiz M, et al. Trapped antihydrogen. Nature. 2010 Dec 2;468(7324):673-6. 12. Bos R, van Der Hoeven JJ, van Der Wall E, et al. Biologic correlates of (18)fluorodeoxyglucose uptake in human breast cancer measured by positron emission tomography. J Clin Oncol. 2002 Jan 15;20(2):379-87. 13. Black RR. Optimization of FDG PET-CT imaging in oncology 2012 (Power point presentation). 14. Hillner BE, Siegel BA, Shields AF, et al. Relationship between cancer type and impact of PET and PET/CT on intended management: findings of the national oncologic PET registry. J Nucl Med. 2008 Dec;49(12):1928-35. 15. Gambhir SS, Czernin J, Schwimmer J, Silverman DH, Coleman RE, Phelps ME. A tabulated summary of the FDG PET literature. J Nucl Med. 2001 May;42(5 Suppl):1S-93S. 16. Nahmias C, Hanna WT, Wahl LM, Long MJ, Hubner KF, Townsend DW. Time course of early response to chemotherapy in non-small cell lung cancer patients with 18F-FDG PET/CT. J Nucl Med. 2007 May;48(5):744-51. 17. Wahl RL, Jacene H, Kasamon Y, Lodge MA. From RECIST to PERCIST: Evolving Considerations for PET response criteria in solid tumors. J Nucl Med. 2009 May;50 Suppl 1:122S-50S. 18. Lucignani G, Paganelli G, Bombardieri E. The use of standardized uptake values for assessing FDG uptake with PET in oncology: a clinical perspective. Nucl Med Commun. 2004 Jul;25(7):651-6. 19. Brix G, Lechel U, Glatting G, et al. Radiation exposure of patients undergoing whole-body dual-modality 18F-FDG PET/CT examinations. J Nucl Med. 2005 Apr;46(4):608-13. |



Wellness
Specialists
1-800-226-2370 - This service is FREE
7:30 AM - 12 AM (ET) Mon-Fri | 9 AM - 12 AM (ET) Sat-Sun