Life Extension Magazine®

Suzanne Somers Uses Novel Stem Cell Therapy During Breast Rejuvenation
For most breast cancer survivors, the only options available to reverse disfigurements are implants or painful, often unsuccessful reconstructive procedures. Suzanne Somers has led the way in finding an alternative to these approaches. In this exclusive interview, Suzanne reveals to William Faloon the intimate, challenging, ultimately successful experiences that helped her reclaim her health, femininity, and well-being using a non-FDA-approved stem cell procedure pioneered in Japan!
Scientifically reviewed by Dr. Gary Gonzalez, MD, in October 2024. Written by: William Faloon.
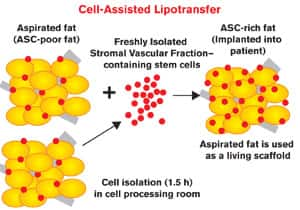
Breast cancer strikes more than 200,000 American women each year.1 About 40,000 die from metastatic disease, leaving 160,000 women alive…but with missing or disfigured breasts.2 For most women, the principal options to reverse the mutilating impact of conventional therapy (lumpectomy or mastectomy plus radiation) are reconstructive surgery using synthetic breast implants or, for women who don't want artificial implants, surgical stripping of abdominal or back muscles which are then used to reconstruct the breast. Both of these reconstructive procedures can involve side effects such as chronic pain and discomfort not only in the breast area, but from hernias and weakness from the donor site of the body, including muscles in the back or abdomen that are surgically removed.3-6 Seldom do any of these conventional reconstruction choices restore the desired sensation, mobility, comfort, and appearance of the original healthy breast. There is, however, another option used by some plastic surgeons in the past called autologous fat grafting, or fat transplantation. This procedure utilizes the patient's own subcutaneous fat tissue from other regions of the body and implants it into the breast. A major concern with this kind of breast restoration is that scientific studies have failed to show clear evidence of long-term viability of the fat transplanted into the breast.7 That's why the concept of enriching transplanted fat with concentrated stem cells offers such incredible potential. Actress Suzanne Somers was diagnosed with breast cancer in 2001. She had a lumpectomy to remove the tumor, followed by intense radiation therapy. For those who don't know, the destructive effects of surgery combined with high-dose radiation can cause severe disfigurement to breast tissues. Even breast conserving/reconstruction surgeries don't always restore and maintain post-treatment breasts anywhere near their original appearance. Those who know Suzanne Somers understand that she does not make important medical decisions in a conventional way. Rather than submitting to traditional breast reconstructive surgery, she scoured the world to identify researchers who were using advanced techniques to improve autologous fat transplantation as a long-term restorative procedure for the breast. Though preliminary, the results thus far have been impressive. Using an advanced technique conceived by Dr. Kotaro Yoshimura in Japan, Suzanne's American surgeon utilized a novel strategy known as Cell-Assisted Lipotransfer.8 Dr. Yoshimura's protocol utilizes autologous adipose-derived stem cells in combination with liposuction techniques. With the Cell-Assisted Lipotransfer strategy, autologous adipose-derived stem cells are used to enhance survival rate of the fat grafts and to reduce postoperative atrophy (shrinkage). Using the novel Cell-Assisted Lipotransfer technology, half the volume of the aspirated fat is processed to isolate the stromal vascular fraction-containing stem cells. During the isolation process, the other half of the aspirated fat is prepared for grafting. Freshly isolated stromal vascular fraction stem cells are attached to the aspirated fat, with the fat acting as a living "scaffold" before transplantation. Finally, the stromal vascular fraction-supplemented fat is injected into the breast. Therefore, stem cell–poor fat is converted to stem cell–rich fat in the preparation process of the injectable material.9,10 The scientific intricacies of this procedure are discussed in an interview with the American surgeon who performed this Cell-Assisted Lipotransfer on Suzanne Somers. In this exclusive interview, Bill Faloon discusses this approach in lay terms with Suzanne and the ramifications it has not only for breast cancer survivors, but also healthy women considering breast implants for cosmetic purposes who may soon have the option of tissue regeneration using their own adipose-derived stem cells.
Bill Faloon (BF): I've always admired the way you detail in your books the battle you waged against cancer and why you refused to accept everything mainstream oncologists insisted on. In The Sexy Years, you disclosed a lot about the treatments you investigated and emotional challenges you confronted. After your lumpectomy, it seemed like the mutilation to your breast was not overly harsh. Was it the follow-up radiation that caused the severe disfigurement that eventually occurred? Suzanne Somers (SS): There should be a book written on the realities of radiation and all the things that are never mentioned beforehand. With radiation, the breast gradually gets flatter and flatter until it looks as though there has been a complete mastectomy. In addition, the asymmetry causes severe pain because in order to look "even" in clothing one side of the bra has to be pulled up so high that it injures the breast and removing the bra becomes excruciating. BF: What is the best way of describing the damage the lumpectomy plus intense follow-up radiation inflicted on your breast? SS: The lumpectomy at first was swollen and didn't look too radical. The treated breast was smaller than the other one but nothing that would make you feel horrified to look at yourself. But when the swelling subsided it was considerably smaller than I had at first realized, and then it began to degrade, gradually losing more and more volume until it became non-existent. Getting dressed became a challenge, and frankly, as a woman with a sexy image in the public arena, it was demoralizing for me. BF: In addition to cosmetic disfigurement, did you experience any mobility problems as a result of the lumpectomy plus intense radiation therapy? SS: I was in constant pain. As I said, in order to wear a bra, the full damaged breast needed to be worn high enough to create evenness. This injured the breast, making bra removal an excruciating experience. Also, as someone who enjoys sex (due to my perfect hormonal balance), having painful breasts was not conducive to that activity. In time, I was always in pain. Something had to be done. BF: You probably investigated a lot of breast reconstruction options. What made you decide against trying any of them? SS: As an avid participant in anti-aging and alternative medicine, the idea of a foreign object in my body was unacceptable. Plus, at the time of my cancer diagnosis, the options presented to me were "implants" in both breasts to assure evenness and symmetry. I absolutely refused to do this. The other option presented to me was the Tram Flap procedure, which was also unacceptable. I have seen the end result of Tram Flap and it is not pretty, plus the recovery time is long and arduous, and it weakens the removal area of the body. It's like trading a headache for a stomach ache. BF: Where did you first learn about the use of stem cells in growing new breast tissue? SS: I interviewed Dr. Robin Smith of the Neostem Company, a stem cell banking company, for my book titled Breakthrough. I was fascinated by the notion that we bank our stem cells while we are healthy and store them cryogenically for later use. I had also asked Dr. Smith if it was possible to use stem cells for a breast regrowth and she said yes, that there were companies focused on this procedure and medical literature demonstrating positive results such as from Dr. Kotaro Yoshimura at the University of Tokyo in Japan. While Dr. Smith made it perfectly clear that there were no current US FDA-approved therapies for breast reconstruction, as an optimist I banked my stem cells with the Neostem Company in 2009, hoping on being able to use these cells one day in the future for this procedure.
BF: Since the Cell-Assisted Lipotransfer procedure used in your breast rejuvenation is not FDA approved, how did you get this done in the United States? SS: In order for Hollywood Presbyterian Hospital to agree to participate in this groundbreaking procedure, they insisted I obtain an Institutional Review Board (IRB) approval qualifying me for a clinical trial. Under this bureaucratic restraint, the FDA would not allow me to use my banked stem cells, only stem cells taken from my fat on the spot. I agreed to work with Dr. Joel Aronowitz, a famous surgeon in Los Angeles with expertise in adult stem cell technology and breast rejuvenation, and together we successfully were able to perform this advanced procedure using enriched adipose-derived stem cells. Other doctors around the country are doing autologous fat transplantation for cosmetic breast surgery, but I am the first to have Dr. Yoshimura's advanced technique utilized, legally, using only my fat enriched with adipose-derived stem cells. BF: Were you able to use your stem cells to regenerate any other areas of your body? SS: After the breast procedure, my doctor requested from NeoStem a portion of my banked adult stem cells that originated in my adult bone marrow but were obtained through my blood. He used these to improve the appearance of the skin on my neck by regenerating the skin, giving me, in essence, a stem cell neck lift, using my fetal banked stem cells. This mix of cells which contain VSELS (very small embryonic-like stem cells) have many regenerative properties. The result is natural new smooth skin, not requiring surgery. These are all great advancements, the best use of scientific breakthroughs, a modern approach to beauty and safer and less invasive than cosmetic surgery. BF: How many women in Japan have had their breasts regenerated using this stem cell technique? SS: Dr. Yoshimura is the pioneer in Asia having completed over 400 procedures using his advanced technique with adipose-derived stem cells in Japan. BF: In lay terms, can you explain how this stem cell breast regeneration therapy is done? SS: In layman terms, they removed the fat by liposuction from my abdominal area. They took that fat and spun it at supersonic speed, separating it into three layers (like a mousse). The first layer was fat, second, blood, third, stem cells. They took the stem cells, cleaned them, separated them, discarding the weak ones, then converged the strongest stem cells back into the fat and whipped those strong stem cells which were now in high concentrations together, and with a "turkey baster" (my terms) injected the stem cell laden fat into my breast until it was of the correct volume. Poof! There it was. BF: So fat removed from the abdomen provides the cells that are then sorted in a laboratory to provide stem cells vibrant enough to regenerate breast tissue? SS: Correct. But the fat can be taken from any part of the body. I would imagine each individual woman would have her favorite places for removal; love handles, thighs, inner thighs. Really the whole procedure is a win, win, win; you get a new real breast, plus you get rid of unwanted fat! BF: Was the removal of fat from your abdomen the first step? SS: Yes and I have to say, liposuction is not for sissies. The recovery from liposuction is the painful part. BF: How long did it take for your doctors to separate the strong stem cells in the laboratory? SS: The cell processing procedure takes about 90 minutes to complete.9 BF: By what route were these stem cells administered back into your body? SS: Dr. Aronowitz can give you the technical terms but I looked at it and thought, "turkey baster!" BF: What should breast cancer patients tell their doctors if they plan on using this stem cell technique to restore their breast tissues? SS: The important thing for women to know is that if they are having a lumpectomy or a mastectomy, it is crucial to maintain the skin and nipple. The mastectomies of yesteryear removed everything, skin and nipple included, so this procedure would not be possible. Today they approach it differently, and if there is no cancer in the nipple or skin it is left intact and that makes a regrowth possible. BF: How would you compare your restored breast to the healthy one you had before the lumpectomy/radiation? SS: If I can brag a little, it is beautiful—high and firm and real and soft and unscarred. Talk about reverse aging. My breasts look like they're from a young woman. I cannot tell you what this has done for me psychologically. I did not do this for aesthetics. I did it for two reasons: medical progress and the positive effect it would have for women of this country, and also to relieve my personal pain and regain symmetry. BF: Why are you the first American to legally benefit from this remarkable technology? SS: Because I researched and persevered. I never gave up. It took me three years to obtain legal permission. I did it right and this is a merger, a true integrative procedure, the best of western and alternative medicine coming together. BF: You could have gone to Japan to have this done, but instead spent a considerable amount of time persuading an American doctor to learn the methodology and then use you as his first patient. Do you think this might wake up our medical authorities about the need to allow therapies from other countries to be used in the United States sooner? SS: Absolutely. Why are Americans spending their life savings to go to far-away places, Dominican Republic, Asia, to name a couple, when we have doctors with knowledge and enthusiasm in our country who want to do these procedures? That is why I wanted to do it here, so it would be an American achievement, and that American women could benefit. We have the best doctors on the planet in the United States, yet in so many cases our doctors have their hands tied behind their backs, legally prohibiting them from being all that they can be. I am hoping my procedure will help in untying those hands. BF: A number of women today are undergoing cosmetic breast augmentation using either saline or silicone implants. There are sometimes surgical complications and many suffer chronic pain, discomfort, and loss of mobility. These artificial implants last about ten years and then the procedure often needs repeating. Do you see the stem cell approach you used eventually replacing the use of cosmetic artificial implants? SS: Yes I do. Maybe this is why obtaining permission was such a long and difficult road. But I ask you, why would any woman ever want to have foreign objects inserted into their bodies when this new procedure is available? Implants are laden with side effects and problems, and degrade health simultaneously. Instead, women could utilize a safe procedure of taking fat from their own body (and who doesn't want a little fat removed) from which they remove the stem cells, and then use their own stem cells (which their body cannot reject) to re-grow their breast and do a better job? BF: A question a lot of our readers are going to ask is when is your next book coming out? SS: How sweet of you to ask. I plan on my next book being a blockbuster on redefining aging and will be published in 2012. I am not revealing the title yet but it's a good one. Hopefully you will grace me with yet another cover on your magazine so everyone will be aware of it. Life Extension® is and has been of vital importance to me, informing me, educating me, and when I am featured in your magazine it allows me to reach the constituency that is most interested in what I have to say. For this new book, I have assembled an incredible group of doctors, some I've interviewed before and some for the first time. As always, writing these books is a learning experience, and I believe the information will inform my global constituency of the incredible advancements that are coming and how to get ready in order to be able to access these advancements. If you have any questions on the scientific content of this article, please call a Life Extension® Health Advisor at 1-866-864-3027. | ||||||
| References | ||||||
| 1. Available at: http://www.cdc.gov/cancer/breast/statistics/index.htm. Accessed Sept. 28, 2011. 2. Available at: http://www.news.cornell.edu/stories/April09/ nyc.breast.cancer.html. Accessed September 28, 2011. 3. Gärtner R, Jensen MB, Nielsen J, Ewertz M, Kroman N, Kehlet H. Prevalence of and factors associated with persistent pain following breast cancer surgery. JAMA. 2009 Nov 11;302(18):1985-92. 4. Tindholdt TT, Tønseth KA. Donor site sensitivity after breast reconstruction with deep inferior epigastric artery perforator flap. Ann Plast Surg. 2009 Aug;63(2):143-7. 5. Kroll SS, Schusterman MA, Reece GP, Miller MJ, Robb G, Evans G. Abdominal wall strength, bulging, and hernia after TRAM flap breast reconstruction. Plast Reconstr Surg. 1995 Sep;96(3):616-9. 6. Available at: http://www.davidgreenspunmd.com/restorative_techniques/other_surgical_options/muscle_flaps. Accessed Oct. 3, 2011. 7. Kaufman MR, Miller TA, Huang C, et al. Autologous fat transfer for facial recontouring: is there science behind the art? Plast Reconstr Surg. 2007 Jun;119(7):2287-96. 8. Matsumoto D, Sato K, Gonda K, et al. Cell-assisted lipotransfer: supportive use of human adipose-derived cells for soft tissue augmentation with lipoinjection. Tissue Eng. 2006 Dec;12(12):3375-82. 9. Yoshimura K, Sato K, Aoi N, Kurita M, Hirohi T, Harii K. Cell-assisted lipotransfer for cosmetic breast augmentation: supportive use of adipose-derived stem/stromal cells. Aesthetic Plast Surg. 2008 Jan;32(1):48-55; discussion 56-7. 10. Yoshimura K, Asano Y, Aoi N, et al. Progenitor-enriched adipose tissue transplantation as rescue for breast implant complications. Breast J. 2010 Mar-Apr;16(2):169-75. |


Wellness
Specialists
1-800-226-2370 - This service is FREE
7:30 AM - 12 AM (ET) Mon-Fri | 9 AM - 12 AM (ET) Sat-Sun