Life Extension Magazine®
An epidemic of autism appears to be underway in the United States. According to several respected leaders in child and adult nutrition from across the United States, the current meteoric rise in autism and autism spectrum disorders (ASD) may well be a direct consequence of significant vitamin D deficiencies in pregnant women and their infants.1-6 And evidence points to vitamin D deficiency as the cause of other debilitating brain conditions as well.5,7-10 This insidious deficiency is readily remedied—yet tragically often missed. For years, Life Extension has been exploring the potentially devastating consequences of vitamin D deficiency, ranging from cardiovascular disease to cancer. Now in this report, Life Extension magazine examines the link between low levels of plasma vitamin D and autism. At the forefront of this research is Dr. John J. Cannell, executive director of the Vitamin D Council and a forensic psychiatrist at Atascadero State Hospital in California. The stunning findings suggest that rampant vitamin D deficiency is causally related to brain dysfunction, and may be readily preventable by adequate supplementation.2-4,11 Autism—What’s Known, What’s Guessed, and What’s Still to be LearnedAutism, or the Autistic Spectrum Disorders (ASD), involves poor social and verbal functioning accompanied by repetitive or “stereotyped” behaviors.12 Symptoms begin sometime in early childhood. Just what the deficits are, when they first become evident, and what causes them are still unknown, though both genetic and environmental factors seem to play major roles.12-14 Similarly, it seems apparent that there are many different developmental conditions that meet at least some of the definitions of autism or ASD.12
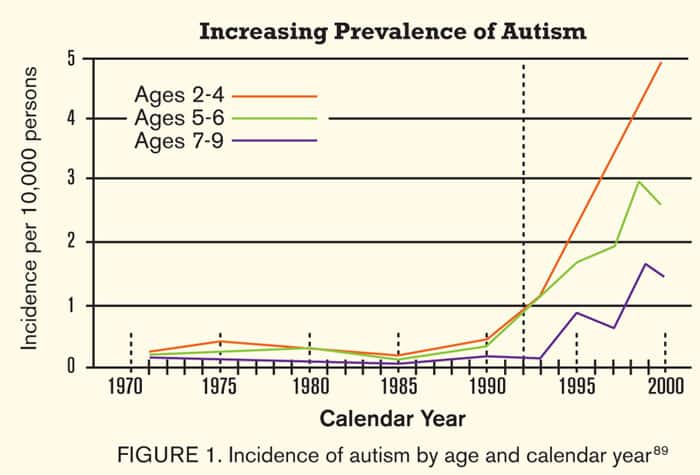
In fact, scientists agree that we actually know very little about this puzzling, multi-faceted, and tragic condition, which ranges in severity from very subtle alterations in social behavior to full-blown developmental delays that may result in placement in long-term care facilities.15-17 What is undeniable is that there has been a marked increase in the number of children being diagnosed with autism over the past two decades, not just in the US but in most industrialized nations.18-21 Some experts argue that this rise is due to increased detection by parents and physicians, as well as changing criteria and diagnostic categories.22-25 By now, however, most agree that the increase is real, and probably represents an interaction of basic genetic tendencies with something new and different in our current turn-of-the-century world.3,19-21 One report showed the incidence of autism rose 30-fold in just seven years.25 This 2006 British study estimated that one in every 86 children met criteria for autism or ASD20—a shocking figure that alone justifies use of the term “epidemic.”3 What is causing this apparent dramatic rise in autism cases? The answer or answers have been elusive, generating heated controversy among (and between) physician groups, other scientists, and many parent groups. Considerable attention has been given to mercury and other environmental toxins that cause oxidative stress,26,27 and scientists are conducting further studies to determine if mercury in the environment and mercury preservatives in vaccines are casually linked to autism. Genetic factors are also important, as demonstrated by high rates of occurrence in other family members, particularly in twin studies.28,29 Today’s consensus identifies both genetic and environmental factors as being relevant to the causes of autism.14,30 The “Vitamin D Deficiency Theory” of AutismWhat possible factors involving both genetics and environment could account for the dramatic change in autism rates in just 20 years? Our genes surely aren’t changing that fast, and while our environment is clearly being altered, no serious scientist suggests that anything radical enough to cause an epidemic of brain dysfunction has taken place in the past two decades. That’s correct, argues Dr. John Cannell, but in fact our behavior with regard to our environment has indeed undergone significant changes—changes that, because of their effects on the vitamin D neurosteroid system, can and do account for many of the observed facts about the autism epidemic.
Dr. Cannell, a widely-published expert on vitamin D’s many-faceted effects,4,31-33 believes that these facts line up in a compelling fashion to implicate vitamin D deficiency and support the “vitamin D deficiency theory” of autism.3 Let’s follow Dr. Cannell’s line of thinking as he lines up the extraordinary evidence that we may be able to stop the autism epidemic in its tracks with simple vitamin D supplementation. Cannell starts with the incredible increase in our understanding of vitamin D’s fundamental contri-butions to human health. Though most people (sadly including many physicians) still associate it only with bone mineralization, we now understand that the active form of vitamin D, called calcitriol, plays an equally important role as a neurosteroid hormone, directly responsible for many elements in brain development and behavior34 (other examples of neurosteroids include the sex hormones estrogen and testosterone, which have effects on the full spectrum of human behaviors). Vitamin D obtained from supplements or sunshine must undergo two biochemical processes before it becomes active. First, it is metabolized by the liver to 25-hydroxyvitamin D, the main circulating form of vitamin D and the only vitamin D metabolite that should be measured to assess vitamin D status. Circulating 25-hydroxyvitamin D then undergoes a final biochemical step to form calcitriol, a potent neurosteroid that controls brain cell growth, and acts on receptor molecules found in brain cells from the first days of embryo formation.35 Because of these potent effects, researchers in 2001 labeled vitamin D the “neglected neurosteroid” and concluded that vitamin D deficiency “should be examined in more detail as a candidate risk factor” for neurodevelopmental disorders such as autism.36 More recently, researchers have suggested that vitamin D, acting as a neurosteroid, offers “neuroprotection, antiepileptic effects, immunomodulation, [impact on] several brain neurotransmitter systems and hormones, as well as regulation of behaviors,”37 stressing the importance of prenatal, neonatal, and postnatal vitamin D supplementation for normal brain functioning.38
But what has happened in the past 20 years that could affect the neurosteroid function of vitamin D and relate it to the explosion of autism cases? Plenty, argues Cannell: put very simply, we have become excessively “sun-phobic” in our efforts to reduce the very real risk of skin cancers.3,39 Couple this with our decreasing natural exposure to sunlight as we’ve moved from agricultural to manufacturing to service-based activities, and you have the “perfect storm” for vitamin D deficiency.1,11 Vitamin D levels in industrialized countries are known to be much lower than those of fully sun-exposed individuals.40 Thus, our behavior has had the paradoxical and unintended consequence of limiting our blood levels of the only known precursor of a vital neurohormone that, in turn, can influence the very organ of behavior itself, the brain.3 What is the evidence to support the vitamin D deficiency theory of autism? A recent review by Dr. Cannell provides a substantial and cogent evidence base,3 starting with the characteristics of the vitamin D neurosteroid system itself. Calcitriol acts as a “molecular switch” in brain tissue, turning on powerful genes that influence brain development. There are about 1,000 genes already known to be targets of calcitriol activity, and that number is growing fast.37,41 But unlike any other vitamin system, the bulk of human vitamin D stores come not from oral intake but from skin production under the influence of sunlight.42,43 As Dr. Cannell notes in his review, “Large populations of pregnant women putting small amounts [of vitamin D] in their mouths—in the form of prenatal vitamins—instead of generating large amounts in their skins, is novel to human brain development;”44 since we no longer get ample sun exposure, we need to pay closer attention to how much vitamin D we do get through our mouths. The case for significant oral supplementation is made even clearer when one considers that skin production of vitamin D is vastly more efficient than oral intake.2 In fact, just 10-40 minutes of summer sunbathing by a fair-skinned adult, notes Cannell, produces about 20,000 units of vitamin D which is presented to the systemic circulation over the next 24 hours45—to get the same amount orally a pregnant woman would have to drink 200 glasses of milk (at 100 IU per glass) or take 50 standard prenatal multivitamins (400 IU per tablet) to realize the same gains!3 But, as Cannell goes on to point out, we’ve been assiduously avoiding sun exposure for the past 20 years, dutifully following AMA guidelines.39 It is precisely during that same 20-year period that we’ve seen the rapid rise in autism rates,14 though as Dr. Cannell acknowledges, “Thousands of other environmental changes occurred during this same time and such associations, on their own, mean little.”3 But there are plenty of additional persuasive arguments supporting the theory. The calcitriol neurohormone system is different from all the body’s other steroid hormone systems. While other steroids are produced directly from the body’s natural store of cholesterol “precursor” compounds, the amount of calcitriol produced is completely dependent on having enough precursor 25-hydroxyvitamin D present in the first place. And brain levels of activated vitamin D, as Cannell observes, “directly depend on the amount of vitamin D the mother makes in her skin or puts in her mouth.”3 Cannell’s dramatic conclusion is that “Human behavior, be it the step into the sun, the step to the supplements, the step into the shade, or the step to the sunscreen, determine brain calcitriol levels.”3 In the case of the human fetus, as we’re about to see, brain calcitriol levels are directly linked to very early cognitive development, with tremendous implications for the developing baby’s brain.
Calcitriol—Nutrient and Neurohormone of Brain DevelopmentA wealth of animal data has emerged demonstrating just how essential calcitriol is in early fetal brain development. Offspring of vitamin D-deficient rats, for example, have abnormal cell growth, structure, and functions in their brains,46-48 excessive and undirected movements,49-52 and subtle alterations in learning and memory.8 Even when the deficiencies occur only late in gestation, they are capable of causing disruptions in adult brain functioning,48 demonstrating the exquisite dependence of brain development on this vital neurohormone. A group of French researchers has in fact found 36 crucial brain proteins that are disrupted when vitamin D is deficient during fetal development,7,53 and others have shown increased brain size and enlargement of the fluid-filled ventricles of the brain9—both abnormalities that are common in autism.54,55 Toxins and Oxidants—Another Important Role for Calcitriol in Autism?What about the apparent importance of toxins and inflammation in autism? Does the vitamin D deficiency theory of autism offer an explanation? Resoundingly yes—for example, it is already known that autistic people have abnormalities in immune functions similar to those that are affected by vitamin D—including increased inflammatory cytokine levels.12,56,57 And we know that much of the ongoing inflammation in autistic brains is the result of oxidative stress12—just where vitamin D’s powerful anti-inflammatory properties are most useful (and most critical if missing).
Calcitriol has nootropic properties—that is, it protects brain tissue by reducing inflammatory cytokine levels which, when elevated, are strongly associated with cognitive impairment.3,58 Calcitriol also protects brain tissue by stimulating production of neuro-trophins, chemicals that combat toxicity from a number of sources including toxic levels of intracellular brain calcium.59 Calcitriol also increases brain levels of glutathione,60,61 a powerful natural antioxidant that is the body’s most important tool for detoxifying and excreting heavy metals and that is rapidly consumed during oxidant stress from toxins and other sources. Cannell argues convincingly that it is especially this calcitriol-induced increase in glutathione levels that can explain the link between autism and heavy metal toxicity.3,62 Heavy metals deplete intracellular glutathione,63 however, animals supplemented with calcitriol show a reduction in iron- and zinc-induced brain injury.64,65 A study by Dr. Jill James sheds further light on the connection between heavy metals, glutathione, and autism. Children with a variant of autism called regressive autism demonstrated a severe imbalance in the ratio of active to inactive glutathione, compared with healthy children. Regressive autism occurs when previously healthy children lose acquired language or behavioral skills and go on to develop autism. Children with regressive autism displayed chronically elevated levels of oxidative stress, which would make them more vulnerable to damaging neurotoxic agents such as heavy metals.66 Vitamin D Interactions—An Answer to the Gender Issue in Autism?The fact that vitamin D metabolism differs markedly under the effects of the sex hormones may go a long way towards explaining yet another puzzling fact about autism, namely its strong predilection for boys over girls.3 For example, researchers in Sweden and in Utah have now shown that estrogen has effects on developing brain tissue that serve to make it more responsive to the neurohormonal growth-stimulating effects of calcitriol—results which suggest that estrogen can enhance any beneficial effects of vitamin D on the brain.67,68 It has been found that estrogen increases the activity of an important vitamin-D-related calcium binding protein in neurons69,70 that plays several important roles during central nervous system development. Though complex, these studies do support the notion that the developing brain of a female fetus, with its predominance of estrogen relative to testosterone, could make more efficient use of available vitamin D than would the brain of a male fetus. In a situation where there was plenty of vitamin D present, such differences would go unnoticed—but introduce the all-too-prevalent maternal vitamin D deficiency state, and the stage is set for possible impairment in boys more commonly than in girls, which is of course precisely the situation we see with autism’s gender discrimination.3 | |||||||





Vitamin D Intake and Cognitive PerformanceIf even some of the damage done by vitamin D deficiency during fetal development is reversible, we’d expect to find that vitamin D supplementation would help reduce autistic symptoms at least to some extent. There aren’t yet many good studies on this subject, but what we know is encouraging. A multivitamin supplementation study of 20 autistic children in 2004 showed improvements in sleep and gastrointestinal problems that are common in autism (that study only provided 150 units of vitamin D per day, which as we’ll see is probably well below the minimum requirement).71 Similar multivitamin studies have shown improvements in cognitive function even in apparently normal schoolchildren, according to one review of 14 separate studies.72 What’s remarkable (and heartbreaking) is that while these studies show very little effect on most of the children evaluated, about 20% of the children had substantial gains in performance.72 This 20% might represent a vitamin D-deficient subgroup of children—a tremendous number if these figures hold nationwide.3 We would also expect that consumption of vitamin D-rich foods by pregnant women would improve cognitive performance in their infants, and indeed Cannell provides evidence that high maternal consumption of fish, rich in vitamin D, is associated with better cognitive outcomes in infants.73,74 Another recent study demonstrated that infants born to mothers with very low seafood intake had higher risks for having low verbal IQs, less well-socialized behaviors, and poorer fine motor and communication skills.75 As Cannell persuasively argues, these deficiencies are “eerily similar to [those found in] autism.”3
Exposure to UV Light—Another Clue?We know that certain brain diseases such as multiple sclerosis are much more common in high latitudes where sunlight is scarce, and many scientists suspect that those conditions are directly related to chronic or seasonal vitamin D deficiencies.1,2,76 A strong positive association between latitude and the prevalence of autism has been reported for groups of children before 1985, which is what we’d expect if autism were related to vitamin D deficiency.3,4 Additional support comes from recent data from the Centers for Disease Control and Prevention (CDC), which found the highest prevalence of autism in New Jersey (the second most northern state in the survey), and the lowest in Alabama.18
One might expect that babies born in late winter would have higher rates of autism if vitamin D deficiency were involved, since their mothers would have spent most of their pregnancies in fairly low-sunlight settings. While one report suggests that late winter birth dates are associated with higher rates of autism,77 the literature isn’t consistent on this topic. Cannell argues that in fact this would be expected if the critical time for the deficiency to cause damage was not only during gestation, but also in early childhood, and indeed animal studies suggest just that.46,50 Lower rates of autism have been found in rural compared with urban areas, further supporting the idea that low sunlight exposure may be a contributor.78 And a fascinating study recently demonstrated that autism rates are substantially higher in geographic areas where precipitation is highest79 (the implication is that people in such areas spend less time outdoors, thereby reducing their vitamin D-producing sun exposure). Finally, air pollution is now known to reduce UV light exposure sufficiently to lower vitamin D levels to the point at which experts are recommending supplementation,80 and one recent study demonstrated an association between air pollution and autism27 (of course this particular association could as easily be due to toxins in the air—demonstrating how much we still have to learn about this mysterious condition). UV-Blocking Skin Pigment—Further Support for the Vitamin D Deficiency TheoryIf fetal vitamin D deficiency is at the root of autism, we should expect to find higher rates of autism among children born to dark-skinned mothers, because melanin, the major skin pigment, is an extremely efficient blocker of UV light.42 As Dr. Cannell points out in his review, studies of this nature are difficult to perform and interpret, though there is limited evidence of higher incidence of autism in American black children.81 Two European studies published in 1995 also showed higher rates of autism among children of dark-skinned immigrants (up to 200-fold higher in one study).82,83 Since some studies suggest that darker-skinned individuals are more likely to be deficient in vitamin D than those with lighter skin tones,84 this provides another compelling reason for those with darker skin tones to diligently monitor their vitamin D status. Summary
There seems to be little doubt that a significant proportion of the epidemic of autism is real, and not just a fluke of over-reporting and over-diagnosis by anxious parents and physicians. As many Life Extension reports have documented, there’s equal certainty that we also face an epidemic of vitamin D deficiency as we steadily move away from old ways that exposed us to more vitamin-D producing sunlight. The theory that the two epidemics are inextricably linked is supported on myriad independent grounds, and as Dr. Cannell himself points out, is readily susceptible to rigorous testing.3 While we are awaiting those results, however, it seems prudent to maximize vitamin D status in pregnant women, infants, and young children and infants, aiming for levels found in humans living in a sun-rich environment, between 50-60 ng/mL (blood testing for 25-hydroxyvitamin is recommended as the only way to make the diagnosis and to assure treatment is adequate and safe).4 One recent study noted, “Supplemental doses of vitamin D and sensible sun exposure could prevent deficiency in most of the general population.”2 Under the leadership of brilliant scientists like Dr. John Cannell, we may be privileged to witness at least the beginning of the end of the scourge of autism among our children. If you have any questions on the scientific content of this article, please call a Life Extension Health Advisor at 1-800-226-2370. | ||||||
| References | ||||||
| 1. Holick MF. The vitamin D epidemic and its health consequences. J Nutr. 2005 Nov;135(11):2739S-48S. 2. Holick MF. High prevalence of vitamin D inadequacy and implications for health. Mayo Clin Proc. 2006 Mar;81(3):353-73. 3. Cannell JJ. Autism and vitamin D. Med Hypotheses. 2008;70(4):750-9. 4. Cannell JJ, Hollis BW. Use of vitamin D in clinical practice. Altern Med Rev. 2008 Mar;13(1):6-20. 5. Johnson S. Micronutrient accumulation and depletion in schizophrenia, epilepsy, autism and Parkinson’s disease? Med Hypotheses. 2001 May;56(5):641-5. 6. Yan J, Feng J, Craddock N, et al. Vitamin D receptor variants in 192 patients with schizophrenia and other psychiatric diseases. Neurosci Lett. 2005 May 20;380(1-2):37-41. 7. Almeras L, Eyles D, Benech P, et al. Developmental vitamin D deficiency alters brain protein expression in the adult rat: implications for neuropsychiatric disorders. Proteomics. 2007 Mar;7(5):769-80. 8. Becker A, Eyles DW, McGrath JJ, Grecksch G. Transient prenatal vitamin D deficiency is associated with subtle alterations in learning and memory functions in adult rats. Behav Brain Res. 2005 Jun 20;161(2):306-12. 9. Eyles D, Brown J, Mackay-Sim A, McGrath J, Feron F. Vitamin D3 and brain development. Neuroscience. 2003;118(3):641-53. 10. Harms LR, Eyles DW, McGrath JJ, Mackay-Sim A, Burne TH. Developmental vitamin D deficiency alters adult behaviour in 129/SvJ and C57BL/6J mice. Behav Brain Res. 2008 Mar 5;187(2):343-50. 11. Holick MF. Deficiency of sunlight and vitamin D. BMJ. 2008 Jun 14;336(7657):1318-9. 12. Ashwood P, Wills S, Van de WJ. The immune response in autism: a new frontier for autism research. J Leukoc Biol. 2006 Jul;80(1):1-15. 13. Lauritsen MB, Pedersen CB, Mortensen PB. Effects of familial risk factors and place of birth on the risk of autism: a nationwide register-based study. J Child Psychol Psychiatry. 2005 Sep;46(9):963-71. 14. London EA. The environment as an etiologic factor in autism: a new direction for research. Environ Health Perspect. 2000 Jun;108 Suppl 3:401-4. 15. Iqbal Z. Ethical issues involved in the implementation of a differential reinforcement of inappropriate behaviour programme for the treatment of social isolation and ritualistic behaviour in an individual with intellectual disabilities. J Intellect Disabil Res. 2002 Jan;46(Pt 1):82-93. 16. Barbaresi WJ, Katusic SK, Voigt RG. Autism: a review of the state of the science for pediatric primary health care clinicians. Arch Pediatr Adolesc Med. 2006 Nov;160(11):1167-75. 17. Karande S. Autism: A review for family physicians. Indian J Med Sci. 2006 May;60(5):205-15. 18. Anon. Prevalence of autism spectrum disorders—autism and developmental disabilities monitoring network, 14 sites, United States, 2002. MMWR Surveill Summ. 2007 Feb 9;56(1):12-28. 19. Atladottir HO, Parner ET, Schendel D, et al. Time trends in reported diagnoses of childhood neuropsychiatric disorders: a Danish cohort study. Arch Pediatr Adolesc Med. 2007 Feb;161(2):193-8. 20. Baird G, Simonoff E, Pickles A, et al. Prevalence of disorders of the autism spectrum in a population cohort of children in South Thames: the Special Needs and Autism Project (SNAP). Lancet. 2006 Jul 15;368(9531):210-5. 21. Blaxill MF. What’s going on? The question of time trends in autism. Public Health Rep. 2004 Nov;119(6):536-51. 22. Croen LA, Grether JK, Hoogstrate J, Selvin S. The changing prevalence of autism in California. J Autism Dev Disord. 2002 Jun;32(3):207-15. 23. Shattuck PT. The contribution of diagnostic substitution to the growing administrative prevalence of autism in US special education. Pediatrics. 2006 Apr;117(4):1028-37. 24. Lauritsen MB, Pedersen CB, Mortensen PB. The incidence and prevalence of pervasive developmental disorders: a Danish population-based study. Psychol Med. 2004 Oct;34(7):1339-46. 25. Hillman RE, Kanafani N, Takahashi TN, Miles JH. Prevalence of autism in Missouri: changing trends and the effect of a comprehensive state autism project. Mo Med. 2000 May;97(5):159-63. 26. Valko M, Morris H, Cronin MT. Metals, toxicity and oxidative stress. Curr Med Chem. 2005;12(10):1161-208. 27. Windham GC, Zhang L, Gunier R, Croen LA, Grether JK. Autism spectrum disorders in relation to distribution of hazardous air pollutants in the san francisco bay area. Environ Health Perspect. 2006 Sep;114(9):1438-44. 28. Le Couteur A, Bailey A, Goode S, et al. A broader phenotype of autism: the clinical spectrum in twins. J Child Psychol Psychiatry. 1996 Oct;37(7):785-801. 29. Muhle R, Trentacoste SV, Rapin I. The genetics of autism. Pediatrics. 2004 May;113(5):e472-86. 30. Herbert MR, Russo JP, Yang S, et al. Autism and environmental genomics. Neurotoxicology. 2006 Sep;27(5):671-84. 31. Cannell JJ, Vieth R, Umhau JC, et al. Epidemic influenza and vitamin D. Epidemiol Infect. 2006 Dec;134(6):1129-40. 32. Cannell JJ, Zasloff M, Garland CF, Scragg R, Giovannucci E. On the epidemiology of influenza. Virol J. 2008;529. 33. Cannell JJ, Hollis BW, Zasloff M, Heaney RP. Diagnosis and treatment of vitamin D deficiency. Expert Opin Pharmacother. 2008;9(1):107-18. 34. Nakagawa K. Effect of vitamin D on the nervous system and the skeletal muscle. Clin Calcium. 2006 Jul;16(7):1182-7. 35. McGrath JJ, Feron FP, Burne TH, Mackay-Sim A, Eyles DW. Vitamin D3-implications for brain development. J Steroid Biochem Mol Biol. 2004 May;89-90(1-5):557-60. 36. McGrath J, Feron F, Eyles D, Mackay-Sim A. Vitamin D: the neglected neurosteroid? Trends Neurosci. 2001 Oct;24(10):570-2. 37. Kalueff AV, Minasyan A, Keisala T, et al. The vitamin D neuroendocrine system as a target for novel neurotropic drugs. CNS Neurol Disord Drug Targets. 2006 Jun;5(3):363-71. 38. Kalueff AV, Tuohimaa P. Neurosteroid hormone vitamin D and its utility in clinical nutrition. Curr Opin Clin Nutr Metab Care. 2007 Jan;10(1):12-9. 39. Anon. Harmful effects of ultraviolet radiation. Council on Scientific Affairs. JAMA. 1989 Jul 21;262(3):380-4. 40. Vieth R. What is the optimal vitamin D status for health? Prog Biophys Mol Biol. 2006 Sep;92(1):26-32. 41. Tavera-Mendoza LE, White JH. Cell defenses and the sunshine vitamin. Sci Am. 2007;297(5):62-5, 68-70, 72. 42. Holick MF. Photosynthesis of vitamin D in the skin: effect of environmental and life-style variables. Fed Proc. 1987 Apr;46(5):1876-82. 43. Poskitt EM, Cole TJ, Lawson DE. Diet, sunlight, and 25-hydroxy vitamin D in healthy children and adults. Br Med J. 1979 Jan 27;1(6158):221-3. 44. Available at: www.vitamindcouncil.org/health/autism/vitamin-d-theory-autism.rtf. Accessed August 19, 2008. 45. Hollis BW. Circulating 25-hydroxyvitamin D levels indicative of vitamin D sufficiency: implications for establishing a new effective dietary intake recommendation for vitamin D. J Nutr. 2005 Feb;135(2):317-22. 46. Feron F, Burne TH, Brown J, et al. Developmental Vitamin D3 deficiency alters the adult rat brain. Brain Res Bull. 2005 Mar 15;65(2):141-8. 47. Ko P, Burkert R, McGrath J, Eyles D. Maternal vitamin D3 deprivation and the regulation of apoptosis and cell cycle during rat brain development. Brain Res Dev Brain Res. 2004 Oct 15;153(1):61-8. 48. O’Loan J, Eyles DW, Kesby J, et al. Vitamin D deficiency during various stages of pregnancy in the rat; its impact on development and behaviour in adult offspring. Psychoneuroendocrinology. 2007 Apr;32(3):227-34. 49. Burne TH, Becker A, Brown J, et al. Transient prenatal Vitamin D deficiency is associated with hyperlocomotion in adult rats. Behav Brain Res. 2004 Oct 5;154(2):549-55. 50. Burne TH, Feron F, Brown J, et al. Combined prenatal and chronic postnatal vitamin D deficiency in rats impairs prepulse inhibition of acoustic startle. Physiol Behav. 2004 Jun;81(4):651-5. 51. Burne TH, O’Loan J, McGrath JJ, Eyles DW. Hyperlocomotion associated with transient prenatal vitamin D deficiency is ameliorated by acute restraint. Behav Brain Res. 2006 Nov 1;174(1):119-24. 52. Kesby JP, Burne TH, McGrath JJ, Eyles DW. Developmental vitamin D deficiency alters MK 801-induced hyperlocomotion in the adult rat: An animal model of schizophrenia. Biol Psychiatry. 2006 Sep 15;60(6):591-6. 53. Eyles D, Almeras L, Benech P, et al. Developmental vitamin D deficiency alters the expression of genes encoding mitochondrial, cytoskeletal and synaptic proteins in the adult rat brain. J Steroid Biochem Mol Biol. 2007 Mar;103(3-5):538-45. 54. Hardan AY, Minshew NJ, Mallikarjuhn M, Keshavan MS. Brain volume in autism. J Child Neurol. 2001 Jun;16(6):421-4. 55. Piven J, Arndt S, Bailey J, et al. An MRI study of brain size in autism. Am J Psychiatry. 1995 Aug;152(8):1145-9. 56. Cantorna MT, Zhu Y, Froicu M, Wittke A. Vitamin D status, 1,25-dihydroxyvitamin D3, and the immune system. Am J Clin Nutr. 2004 Dec;80(6 Suppl):1717S-20S. 57. Cantorna MT, Mahon BD. Mounting evidence for vitamin D as an environmental factor affecting autoimmune disease prevalence. Exp Biol Med (Maywood). 2004 Dec;229(11):1136-42. 58. Moore ME, Piazza A, McCartney Y, Lynch MA. Evidence that vitamin D3 reverses age-related inflammatory changes in the rat hippocampus. Biochem Soc Trans. 2005 Aug;33(Pt 4):573-7. 59. Cohen-Lahav M, Shany S, Tobvin D, Chaimovitz C, Douvdevani A. Vitamin D decreases NFkappaB activity by increasing IkappaBalpha levels. Nephrol Dial Transplant. 2006 Apr;21(4):889-97. 60. Kalueff AV, Eremin KO, Tuohimaa P. Mechanisms of neuroprotective action of vitamin D(3). Biochemistry (Mosc). 2004 Jul;69(7):738-41. 61. Garcion E, Thanh XD, Bled F, et al. 1,25-Dihydroxyvitamin D3 regulates gamma 1 transpeptidase activity in rat brain. Neurosci Lett. 1996 Oct 4;216(3):183-6. 62. Garcion E, Wion-Barbot N, Montero-Menei CN, Berger F, Wion D. New clues about vitamin D functions in the nervous system. Trends Endocrinol Metab. 2002 Apr;13(3):100-5. 63. Quig D. Cysteine metabolism and metal toxicity. Altern Med Rev. 1998 Aug;3(4):262-70. 64. Chen KB, Lin AM, Chiu TH. Systemic vitamin D3 attenuated oxidative injuries in the locus coeruleus of rat brain. Ann NY Acad Sci. 2003 May;993:313-24. 65. Lin AM, Chen KB, Chao PL. Antioxidative effect of vitamin D3 on zinc-induced oxidative stress in CNS. Ann NY Acad Sci. 2005 Aug;1053:319-29. 66. James SJ, Cutler P, Melnyk S, et al. Metabolic biomarkers of increased oxidative stress and impaired methylation capacity in children with autism. Am J Clin Nutr. 2004 Dec;80(6):1611-7. 67. Fan X, Warner M, Gustafsson JA. Estrogen receptor beta expression in the embryonic brain regulates development of calretinin-immunoreactive GABAergic interneurons. Proc Natl Acad Sci USA. 2006 Dec 19;103(51):19338-43. 68. Taylor H, Quintero EM, Iacopino AM, Lephart ED. Phytoestrogens alter hypothalamic calbindin-D28k levels during prenatal development. Brain Res Dev Brain Res. 1999 May 14;114(2):277-81. 69. Christakos S, Dhawan P, Benn B, et al. Vitamin D: molecular mechanism of action. Ann NY Acad Sci. 2007 Nov;1116:340-8. 70. Onishi T, Shintani S, Wakisaka S, Ooshima T. Relationship of vitamin D with calbindin D9k and D28k expression in ameloblasts. Arch Oral Biol. 2008 Feb;53(2):117-23. 71. Adams JB, Holloway C. Pilot study of a moderate dose multivitamin/mineral supplement for children with autistic spectrum disorder. J Altern Complement Med. 2004 Dec;10(6):1033-9. 72. Schoenthaler SJ, Bier ID, Young K, Nichols D, Jansenns S. The effect of vitamin-mineral supplementation on the intelligence of American schoolchildren: a randomized, double-blind placebo-controlled trial. J Altern Complement Med. 2000 Feb;6(1):19-29. 73. Oken E, Wright RO, Kleinman KP, et al. Maternal fish consumption, hair mercury, and infant cognition in a U.S. Cohort. Environ Health Perspect. 2005 Oct;113(10):1376-80. 74. Sioen I, De Henauw S, Van CJ. Evaluation of benefits and risks related to seafood consumption. Verh K Acad Geneeskd Belg. 2007;69(5-6):249-89. 75. Hibbeln JR, Davis JM, Steer C, et al. Maternal seafood consumption in pregnancy and neurodevelopmental outcomes in childhood (ALSPAC study): an observational cohort study. Lancet. 2007 Feb 17;369(9561):578-85. 76. Holick MF. Vitamin D: A millenium perspective. J Cell Biochem. 2003 Feb 1;88(2):296-307. 77. Stevens MC, Fein DH, Waterhouse LH. Season of birth effects in autism. J Clin Exp Neuropsychol. 2000 Jun;22(3):399-407. 78. Williams JG, Higgins JP, Brayne CE. Systematic review of prevalence studies of autism spectrum disorders. Arch Dis Child. 2006 Jan;91(1):8-15. 79. Available at: http://www.nber.org/papers/w12632. Accessed August 20, 2008. 80. Agarwal KS, Mughal MZ, Upadhyay P, et al. The impact of atmospheric pollution on vitamin D status of infants and toddlers in Delhi, India. Arch Dis Child. 2002 Aug;87(2):111-3. 81. Croen LA, Grether JK, Selvin S. Descriptive epidemiology of autism in a California population: who is at risk? J Autism Dev Disord. 2002 Jun;32(3):217-24. 82. Goodman R, Richards H. Child and adolescent psychiatric presentations of second-generation Afro-Caribbeans in Britain. Br J Psychiatry. 1995 Sep;167(3):362-9. 83. Gillberg C, Schaumann H, Gillberg IC. Autism in immigrants: children born in Sweden to mothers born in Uganda. J Intellect Disabil Res. 1995 Apr;39 ( Pt 2)141-4. 84. Jacobs ET, Alberts DS, Foote JA, et al. Vitamin D insufficiency in southern Arizona. Am J Clin Nutr. 2008 Mar;87(3):608-13. 85. Vieth R, Cole DE, Hawker GA, Trang HM, Rubin LA. Wintertime vitamin D insufficiency is common in young Canadian women, and their vitamin D intake does not prevent it. Eur J Clin Nutr. 2001 Dec;55(12):1091-7. 86. Brot C, Vestergaard P, Kolthoff N, et al. Vitamin D status and its adequacy in healthy Danish perimenopausal women: relationships to dietary intake, sun exposure and serum parathyroid hormone. Br J Nutr. 2001 Aug;86 Suppl 1S97-103. 87. Heaney RP. The Vitamin D requirement in health and disease. J Steroid Biochem Mol Biol. 2005 Oct;97(1-2):13-9. 88. Available at: http://www.cps.ca/english/statements/II/FNIM07-01.htm#SUMMARY. Accessed August 19, 2008. 89. Madsen KM, Lauritsen MB, Pedersen CB, et al. Thimerosal and the occurrence of autism: negative ecological evidence from Danish population-based data. Pediatrics. 2003 Sep;112(3 Pt 1):604-6. |


Wellness
Specialists
1-800-226-2370 - This service is FREE
7:30 AM - 12 AM (ET) Mon-Fri | 9 AM - 12 AM (ET) Sat-Sun