Life Extension Magazine®
Predicting which nutrients will emerge as life-saving superstars can be challenging. For example, a vitamin introduced just a decade ago is demonstrating profound anti-aging effects that extend far beyond its original indications. Based on an abundance of positive findings, scientists have developed a more cost-effective form of this nutrient that enables it to stay in the body much longer than before. The incredible news is that maintaining constant levels of this nutrient not only protects against atherosclerosis, but may reverse arterial calcification as well! A wealth of studies published in 2008 reveals this same nutrient possesses anticancer properties while suppressing factors involved in common age-related diseases.1-15 A hallmark of normal aging involves calcification in soft tissues throughout the body such as heart valves, glands, and blood vessels.16-18 One might erroneously think that dietary calcium is a culprit behind pathological calcification processes. The opposite is true. When rabbits are fed calcium-deficient diets, calcification rates rise by 2.7-fold. Calcium-supplemented diets, on the other hand, reduce calcification by 62%.19 The reason for this contradiction is that in response to a deficit of calcium in the blood, the body excessively robs our bones20 and saturates soft tissues with calcium. As we age, we lose our ability to regulate calcium balance and then suffer the lethal consequences of systemic calcification. It is encouraging to know that a low-cost nutrient (vitamin K) can quickly restore calcium homeostasis. An Extreme Example
Warfarin (Coumadin®) is an anticoagulant drug that inhibits normal vitamin K function in the body. The alarming result of vitamin K impairment is rapid development of osteoporosis and arterial calcification.21,22 Vitamin K is absolutely essential for regulating calcium balance in the body. A deficiency of vitamin K status causes brittle bones and a vascular system that hardens to a state of poor functionality.23-26 People who take Coumadin® suffer more osteoporotic fractures21 and show substantially more abnormal calcium deposition in other areas, such as heart valves—twice as much as non-Coumadin® takers.22 The fact that these pathological changes are allowed to occur in humans prescribed warfarin is unconscionable given the knowledge about the value of low-dose vitamin K supplementation, even in patients at high risk for abnormal arterial blood clots. How Dangerous is Arterial Calcification?
Atherosclerosis is the leading cause of disability and death in civilized societies. Many factors are involved in its initiation and progression.27,28 Homocysteine or oxidized low-density lipoprotein (LDL) can initially damage the inner arterial lining (the endothelium).29 To repair this damage, the endothelium produces collagen that forms a cap over the injury site. These endothelial collagen caps attract calcium that accumulates (calcifies) and forms a hard material resembling bone. This is why atherosclerosis is sometimes referred to as “hardening of the arteries.” Calcification of the coronary arteries markedly increases heart attack risk.30 A substantial volume of studies shows that insufficient vitamin K2 accelerates arterial calcification.31 A new study shows that restoring vitamin K2 reverses arterial calcification.49 Vitamin K functions to keep calcium in the bone and prevent its buildup in the arteries.23-26,28,31 If that is all vitamin K did, it would be one of the most important nutrients for aging humans to take. Newly published research, however, indicates vitamin K2 possesses a host of additional benefits.
Combating Rheumatoid ArthritisRheumatoid arthritis is an autoimmune disease that causes chronic inflammation in the joints and other organs in the body. Those afflicted with rheumatoid arthritis have startlingly high rates of cardiovascular diseases.33 In a study published in June 2008, Japanese scientists found that vitamin K2 inhibited the proliferation of synovial cells and prevented the development of collagen-induced rheumatoid arthritis in the rat model. The scientists concluded that vitamin K2 may represent a new agent for the treatment of rheumatoid arthritis in combination with other anti-inflammatory drugs.34 A recent human study showed that the use of vitamin K2 alone or in combination with bisphosphonate drugs (like Fosamax®) for treatment of osteoporosis in patients with rheumatoid arthritis may inhibit osteoclast induction via decreases in levels of inflammatory mediators.35 Excess osteoclast activity depletes bone mineral density. Enhancing the Bone-Building Effects of Fosamax®Americans afflicted with osteoporosis or low bone mineral density scores are sometimes prescribed drugs like Fosamax® or Actonel®. Side effects from these drugs sometimes preclude their long-term use. Japanese patients are often prescribed high doses of vitamin K2 instead of drugs. Published studies demonstrate the ability of vitamin K2 by itself to halt the loss of bone mineral density.23,36,37 A study published in May 2008 used both Fosamax® and vitamin K2 in postmenopausal women in Japan for one year. The results showed that addition of vitamin K2 led to a greater increase of femoral neck bone density, compared with Fosamax® alone. The doctors confirmed the specific bone-protecting mechanism unique to vitamin K2, a finding that had been established in previous studies.38 Vitamin K2 Reduces Prostate Cancer RiskDoctors in Germany conducted a study examining the relationships between dietary intake of vitamin K1 and K2 on the development of prostate cancer in 11,319 men over an 8.6-year follow-up.4 Compared with the lowest intake of vitamin K2, men with the highest vitamin K2 dietary consumption showed a 63% reduced incidence of advanced prostate cancer. Intake of vitamin K1 was not related to prostate cancer incidence in this 2008 study.4 Improving Fracture Healing Rates
Skeletal fractures cause significant disability and there is growing interest in identifying methods to accelerate the healing time of broken bones. The synergistic effect of vitamin D3 and vitamin K2 in preventing osteoporosis has been documented in clinical practice.39 Up until now, however, there were no reports investigating if these nutrients could enhance fracture healing. An in vitro study published in January 2008 showed that combining vitamins D3 and K1 favorably modulated the proliferation and differentiation of cells required to heal bone. This led the doctors to conclude that these nutrients taken together offer clinicians a promising low-cost strategy for laying down new bone material.39 Vitamin K in Cancer TreatmentVitamin K2 induces differentiation and apoptosis in a wide array of human cancer cell lines. A search of PubMed reveals studies published in 2008 that discuss the role of different forms of vitamin K in the treatment of cancer.1-15 A goal of cancer researchers is to identify compounds that cause cancer cells to self-destruct. Vitamin K2 has been shown to induce apoptosis (cell destruction) in leukemia cells in vitro. A study published in July 2008 identified yet another pathway by which vitamin K2 causes the degradation (via autophagy) of leukemia cells’ own components. The scientists noted that apoptosis and autophagy in leukemia cells could be simultaneously induced by vitamin K2.8 In the laboratory, vitamin K2 demonstrates inhibitory effects against myeloma and lymphoma, suggesting possible applications for individuals fighting these all too common cancers.40 Infection with the hepatitis B or C virus is a major risk factor in developing primary liver cancer, known medically as hepatocellular carcinoma. It can also occur in those who do not have hepatitis. A study published in the Journal of the American Medical Association showed that in those with viral-induced liver cirrhosis, less than 10% of patients given vitamin K2 developed liver cancer. In similar patients not given vitamin K2, a startling 47% developed primary liver cancer.41 Vitamin K2 decreased the risk of hepatocellular carcinoma to about 20% compared with the control group. In a study published in early 2008, 61 primary liver cancer patients who were in remission after treatment were separated into two groups. One group was given supplemental vitamin K2. After one year, only 13% of the group that received K2 experienced recurrence of liver cancer, compared with 55% of the group who did not receive K2. Three-year survival in the vitamin K2-supplemented group was 87% compared with 64% in the group not receiving the vitamin K2.42 In 2007, scientists identified specific anticancer mechanisms for vitamin K2, including inhibition of proinflammatory nuclear factor-kappa B (NFkB) that is often over-expressed in cancer cells.43 Tumor cells use proinflammatory factors to develop survival mechanisms that thwart conventional attempts to eradicate them. Drugs like Coumadin® that antagonize vitamin K do more than cause bone loss and arterial calcification. In a model of melanoma in mice, the oral administration of anticoagulant drugs that antagonize vitamin K “drastically promoted metastasis.” The promotion of metastasis was almost completely suppressed by the pre-administration of vitamin K3, suggesting that these anticoagulant drugs promote metastasis by specifically antagonizing vitamin K.44 While vitamins K1 and K2 are safe and effective, vitamin K3 is potentially toxic and its use has been limited to treating aggressive cancers. A study published in early 2008 identified several specific mechanisms by which vitamin K3 damages pancreatic cancer cells, leading the researchers to state that, “the action of vitamin K3 may lead to a favorable outcome against pancreatic cancer.”7
Vitamin K3 Drug Effective Against End-Stage Prostate CancerApatone® is a drug consisting of vitamin C and vitamin K3. It has been granted orphan drug status by the FDA to treat advanced bladder cancer. Apatone® selectively targets tumors by entering cancer cells as readily as glucose. It then suppresses inflammatory responses (such as those induced by nuclear factor-kappa B) that cancer cells use to escape destruction by chemotherapy agents. Vitamin K3 is being clinically tested as an agent to administer prior to chemotherapy to decrease the resistance tumor cells develop to chemo drugs. In March 2008, the results of a study were published on prostate cancer patients who had failed standard therapy and were given the drug Apatone® at a dose that equaled 5,000 mg of vitamin C and 50 mg of vitamin K3. The results showed that PSA velocity decreased and the time it took PSA to double increased in 13 of 17 patients. Of the 15 patients who continued on Apatone®, only one death occurred after 14 months of treatment. The doctors concluded, “Apatone® showed promise in delaying biochemical progression in this group of end stage prostate cancer patients.”5 Based on the plethora of studies published in 2008, vitamins K2 and K3 have emerged as intriguing agents in both cancer prevention and treatment.
| |||||||||||





Cancer Patients Prone to Vitamin K Deficiency
Many patients with advanced cancer are malnourished from the disease or from the use of chemotherapy, which may cause nausea and poor appetite. Ten percent of these patients experience hemorrhagic (bleeding) side effects.45 Since vitamin K deficiency causes bleeding, doctors conducted a study to establish vitamin K status in advanced cancer patients receiving palliative care. The findings were published in April 2008 and showed that 22% of these cancer patients were deficient in vitamin K1, which is considered below the lower limit of the reference range (below 0.33 nmol/L of blood).45 A startling 78% of these cancer patients showed evidence of a functional vitamin K deficiency, as indicated by elevated levels of an under-carboxylated protein that vitamin K normally carboxylates. The doctors concluded that patients with advanced cancer are prone to vitamin K deficiency and that blood tests should be done to monitor vitamin K status before an increased risk of bleeding develops.45 Advantage of Vitamin K2 Over K1In nature, vitamin K is found in two forms: vitamin K1, which occurs in leafy green vegetables; and vitamin K2, which exists in organ meats, egg yolks, dairy products, and particularly in fermented products such as cheese and curd. While some ingested K1 is converted to K2 in the body, significant benefits occur when vitamin K2 itself is supplemented.46
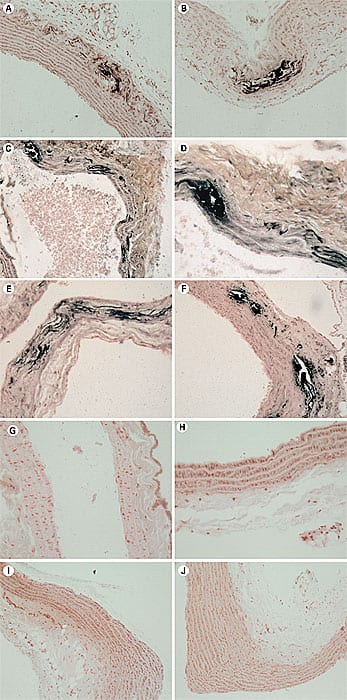
The absorption of K2 into the bloodstream is relatively efficient, whereas relatively little K1 is absorbed from plant foods.47 The kinds of foods rich in K2 in the Western world (organ meats, eggs, and dairy) should not be eaten in excess. Japanese who eat large quantities of a fermented soybean food called natto have lower rates of heart disease and osteoporosis.36,48 Natto is naturally rich in vitamin K2, but most people in Western worlds find it unpalatable. In a fascinating study, rats given vitamin K1 plus warfarin were not protected against arterial calcification. The scientists fed rats a diet containing warfarin plus vitamin K1, vitamin K2 (MK-4), or both vitamin K1 and K2 (MK-4). None (0%) of the rats that received vitamin K2 developed arterial calcification, while 100% of the rats that received vitamin K1 without vitamin K2 displayed calcification in the aorta and carotid arteries!49 A more recent study showed that higher-dose vitamin K decreased arterial calcium content by 50% in rats.49 What makes this finding so remarkable is that most people over age 30–40 already have some degree of arterial calcification and up until now have had no means to reverse it. One of the most convincing studies showing the cardioprotective benefits of K2 can be seen in a large-scale, well-controlled trial called the Rotterdam Heart Study—a Dutch trial that tracked 4,800 participants for seven years.46 The Rotterdam Heart Study revealed that participants who ingested the greatest quantities of vitamin K2 in their diet experienced a 57% reduction in death from heart disease compared with people who ingested the least. The same relationship did not hold for vitamin K1.46 Higher intakes of vitamin K2 in this study corresponded to less calcium deposition in the aorta (an indirect measure of atherosclerosis), whereas participants who ingested less K2 were more likely to show moderate or severe calcification.46 The size and quality of the Rotterdam Heart Study gave credibility to the powerful association between vitamin K2 dietary intake and heart disease and suggests that vitamin K2 may confer cardiovascular benefits by inhibiting arterial calcification.46 Scientists are now intensely interested in finding ways to halt the accumulation of coronary calcium, since they know that it comprises a significant portion of atherosclerotic plaque. They may have to look no further than a new form of vitamin K that remains biologically active in the body for more than 24 hours! Far Greater Absorption of Vitamin K2 Into Cells
A study compared the absorption and arterial wall uptake of vitamin K1 and K2. This study is important because of the large body of epidemiological data showing significant reductions in heart attack risk in those ingesting high amounts of vitamin K2. The results of this study showed that vascular cells preferentially take up vitamin K2 compared with vitamin K1. The poor absorption of K1 into vascular cells helps explain why K1 has not conferred significant protection against heart disease.32 The scientists who conducted this study next evaluated the effect of the K2 absorbed into vascular smooth muscle cells. Their findings documented that K2 enables the formation of smooth vascular muscle without nodules, such nodules that can protrude through into the endothelium and contribute to arterial blockage and atherosclerosis.50 The Long-Acting Form of Vitamin K2There are two forms of vitamin K2 that have demonstrated remarkable benefits in published scientific studies. The MK-4 form of vitamin K2 is the most rapidly absorbed and has proven clinical benefits. Yet MK-4 remains active in human blood for only a few hours after ingestion. The MK-4 form shows activity as an anti-atherosclerotic, has anti-tumor effects in some cancer cells, and helps to aid in bone formation activity.51-56 The MK-7 form of vitamin K2, on the other hand, remains bioavailable in the human body many days after ingestion and is the form found naturally in natto (fermented soybeans).57 In a human clinical trial, comparisons of bioavailability after ingestion of vitamins K1 and K2 (MK-7 form) were performed. The results showed that over a 24-hour period, MK-7 was present in the blood 2.5-fold better than K1. Over a 96-hour period, MK-7 was six-fold better than K1.57 (Shown to the right on Figure 1.) A dose-response study was done where healthy volunteers received increasing doses of K1 and K2 (MK-7). The results showed no effect of K1 observed 24 hours after a 200 microgram dose, whereas 100 micrograms of K2 provided optimal vitamin K blood levels over a 24-hour period.57 (Shown to the right on Figure 2.) A third clinical study compared K1 with K2 (MK-7 form) at the same dose over a six-week period. Compared with K1, the level of MK-7 form of vitamin K2 was seven- to eight-fold higher in the blood and there was no cumulative effect of K1! This suggests that MK-7 is more efficacious than K1.57 (Shown to the right on Figure 3.) Efficacy of the MK-7 Form on a Marker of Bone HealthA sensitive indicator of vitamin K status in the body is the amount of activated osteocalcin in the blood.58 Osteocalcin is produced mainly by osteoblasts (bone-forming cells) and when activated by vitamin K, has properties that allow calcium and other minerals to be laid down into the bone, promoting bone density. When compared with K1, the MK-7 form of vitamin K2 was found to be three times more effective in promoting activated osteocalcin, indicating greater benefits for the bone.57 High bone turnover is associated with bone loss. One aim of osteoporosis prevention is to decrease bone turnover. A higher amount of inactivated (under-carboxylated) osteocalcin is correlated with reduced bone mass. When administered to a group of study subjects, MK-7 was shown to decrease bone turnover and increase bone density.59 A variety of studies done in humans and animals provides much support for the use of MK-7 in the prevention of osteoporosis.59-62 It should be noted that these markers not only provide a partial indication of overall bone health but hint of a strong protective effect of the MK-7 form of vitamin K2. | ||||||||||

Can Vitamin K be Used in Those Taking Coumadin®?
Patients prescribed anticoagulant drugs like warfarin (Coumadin®) are often advised to avoid consuming foods that contain vitamin K. The theory behind this is that dietary vitamin K can circumvent the anticoagulant properties of the drug. The horrific downside to this vitamin K deficit is arterial and valvular calcification along with weakened bones, as previously described. Life Extension has suggested that patients taking anticoagulant drugs like warfarin ask their doctors if they can take a moderate dose of vitamin K2 to not only provide the body with this vital nutrient, but to also better stabilize the anticoagulant effects of the drug. Published studies indicate that when warfarin-treated patients take consistent amounts of vitamin K, blood indicators of coagulation (such as the international normalized ratio or INR) become more stable, which is of critical importance. The reason that consistency is so important is that an INR reading too low places the patient at risk for developing a blood clot inside an artery or vein, whereas an INR ratio that is too high predisposes the patient to abnormal bleeding (internal and external). Maintaining the INR within a narrow therapeutic range is a challenge for many doctors. In fact, when a patient’s INR level gets too high, the antidote is an injection of vitamin K to quickly bring it down to a safe range.
In a recent study in healthy individuals, Coumadin® was administered to elevate INR to 2.0, which is double the normal value for healthy adults. A higher INR means the blood is less able to clot. At a dose of 95 micrograms of MK-7, the INR dropped from 2.0 to 1.7.56 Based on what we now know about vitamin K and warfarin, a doctor might consider increasing the amount of warfarin to bring the INR back into the desired range, while enabling the patient’s vascular and skeletal systems to benefit from vitamin K. If you are taking anticoagulant drugs, do not initiate vitamin K without your doctor’s approval. It is important for your INR levels to be carefully monitored during the first two months of combining moderate-dose vitamin K with warfarin. Please know that enlightened doctors are increasingly expressing concern about the adverse effects of long-term vitamin K deficits in warfarin-treated patients.
Do Healthy People Have to Worry About Taking Too Much Vitamin K?While vitamin K is required for healthy blood clotting, taking too much does not increase the risk of an abnormal clot. The reason is that vitamin K causes a complete chemical conversion (carboxylation) of coagulation-dependent proteins in the body to put them into an active form. Once these coagulation proteins are acted upon by vitamin K, they are 100% carboxylated. If you take additional vitamin K, nothing will happen because all of the coagulation proteins that can be carboxylated are already carboxylated. It is not possible to over-carboxylate coagulation proteins because they are already 100% carboxylated by the vitamin K you took. Patients predisposed to abnormal blood clots, such as those with mechanical heart valves, atrial fibrillation, or prothrombotic factors in the blood are prescribed drugs like warfarin that interfere with the carboxylation of coagulation proteins. It is only in patients taking these anticoagulant drugs that the dose of vitamin K and the drugs need to be closely measured to achieve the optimal therapeutic INR range (usually around 2.5 in people who take warfarin). To demonstrate the safety of vitamin K2, people living in the Japanese regions where natto is regularly eaten have several-fold greater blood levels of vitamin K2 (MK-7).36 The effect of high amounts of vitamin K in the blood is less osteoporosis, fewer bone fractures, and fewer heart attacks.23,30,36,46,63-65 Vitamin K and AgingAs we age, calcium deposits tend to accumulate in soft tissues throughout our bodies.
Doctors performing autopsies on elderly people used to comment that it appeared that the soft tissues in these once supple bodies had turned to stone. These doctors were referring to the systemic calcification occurring virtually everywhere except the skeleton. Systemic calcification means that calcium that is supposed to be deposited in the bones is instead being lodged in soft tissues where it does not belong. Many age-related diseases can be linked to calcification including kidney stones, arthritis, cataracts, heart valve insufficiency, bone fractures, wrinkled skin, bone spurs, senility and, of course, coronary atherosclerosis. Restoring optimal vitamin K status may help to protect against all of these disorders. Osteoporosis is a classic age-related disease. A systemic review of 13 randomized controlled human trials that gave adults either vitamin K1 or K2 supplements for at least six months found that except for one, supplemental vitamin K1 or K2 reduced bone mass loss. Vitamin K2 in particular was associated with increased bone mineral density.66 In all trials to evaluate fracture risk, vitamin K2 was most effective. It reduced the risk of vertebral fractures by 60%, hip fractures by 77%, and all non-vertebral fractures by an astounding 81%.66 As can be seen on the chart on this page, higher ingestion of vitamin K results in a 26% reduction in all-cause mortality.46 Based on the enormity of published scientific studies, maintaining optimal vitamin K status would appear to be an essential component of a comprehensive anti-aging program. Which Form and What Dose of Vitamin K is Optimal?There are scientific studies that document the benefits of vitamin K1, vitamin K2 (in the MK-4 form), and vitamin K2 (in the MK-7 form). Based on a careful evaluation of the various forms of vitamin K, and the wide range of dosage safety and efficacy data that have been established, it would appear ideal for health-conscious individuals to consume all three of these vitamin K forms. The significantly longer-acting MK-7 makes this form of vitamin K2 essential, whereas an abundance of animal and human data confirms significant health benefits of the MK-4 form of vitamin K2, as well as vitamin K1.
Fortunately, all these forms of vitamin K are relatively low-cost and can readily fit into most consumers’ supplement budget. According to the US Department of Agriculture, it used to appear that Americans consumed many times the recommended daily requirement for vitamin K in their diets. But improved analytical methods show that vitamin K is not as abundant in the diet as once thought. The RDA for vitamin K1 and K2 combined is 65 micrograms per day for adult females and 80 micrograms per day for adult males. While these amounts may be enough to enable blood to properly clot, they fall way below the levels found in published studies needed to protect against age-related diseases. One reason for the confusion over optimal vitamin K intake is that only a small amount is needed for blood to properly clot, whereas much higher levels are needed to protect against osteoporosis and calcification of soft tissues (including arteries). Consuming 100 micrograms of the MK-7 form of vitamin K2 may in itself provide optimal systemic vitamin K saturation, yet one cannot ignore the documented benefits of consuming higher amounts of vitamin K1 and the MK-4 form of vitamin K2. With the availability of cost-effective MK-7, the total vitamin K potencies needed to be ingested can be drastically reduced. Remember that compared with other forms of vitamin K, the MK-7 form of vitamin K2 remains in the bloodstream longer and reaches levels seven- to eight-fold higher.57 This means that just 100 micrograms of MK-7 can provide greater benefits than far higher potencies of other forms of vitamin K1 and K2. SummaryVitamin K was discovered in 1929 and it was initially thought to only be required for healthy blood clotting. Over the past 10 years, a large body of research has focused on new areas of vitamin K metabolism, which include its critical effects on bone and vascular health; cell growth, regulation, migration, proliferation, and apoptosis; immune support; and suppression of chronic inflammatory factors. Most conventional doctors wallow in an egregious state of ignorance regarding vitamin K and have no idea of its critical importance to their aging patients. Fortunately, people not taking anticoagulant drugs can safely take doses of vitamin K that exceed the miniscule levels the government says we need. New forms of vitamin K enable health-conscious individuals to take this nutrient just once a day and enjoy sustained 24-hour benefits. When Life Extension introduced its members to vitamin K almost a decade ago, it was difficult to know that it would prove to be as effective as recent studies have demonstrated. It is gratifying to know that most Life Extension members have obtained the broad-spectrum protection of this too often overlooked nutrient. On the flipside, there appears to be an epidemic of age-related disorders in the general population related to less than optimal intake of vitamin K. If you have any questions on the scientific content of this article, please call a Life Extension Wellness Specialist at 1-800-226-2370. | |||||||
| References | |||||||
|



Wellness
Specialists
1-800-226-2370 - This service is FREE
7:30 AM - 12 AM (ET) Mon-Fri | 9 AM - 12 AM (ET) Sat-Sun