Life Extension Magazine®
 |
I’ll never forget an experience I had at a medical conference 14 years ago. A renowned scientist persistently asked me to sell him the hormone leptin.
When given to obese mice, leptin caused weight loss of 40% after 33 days.
In human terms, that equates to a 250-pound person shrinking to 150 pounds in a short time. The problem was that leptin did not work in humans, if they were not leptin-deficient to begin with.1
This obese scientist kept badgering me because he thought I knew how to get leptin. When I repeatedly said it would not work for him, he asked me why it would not work. Back in 1994, I did not know that answer.
In a breakthrough that may reverse today’s epidemic of obesity, a natural compound has been discovered that circumvents the molecular factors involved in obesity … including a phenomenon known as “leptin-resistance.”2-4 This means that for the first time, humans can benefit from their own leptin because it can now enter cells and do what it did for obese mice … induce massive weight loss!
In a recent controlled study, humans taking this new compound lost 28 pounds over a 10-week period compared to less than 3 pounds in the placebo group.5 Unlike other weight loss studies that mandate at least some moderation in food intake, these study participants did not alter their diet in any way.
Equally remarkable are results showing the same mechanisms that enable this compound to remove body fat also lower heart attack risk factors like LDL,5,6 glucose7,8 and C-reactive protein.5
In this article, I will discuss scientific findings showing how this new compound produces more impressive weight loss results than any other drug, nutrient or hormone in medical history.
Scientists have identified specific factors that cause aging people to accumulate unwanted fat pounds. The problem has been that up until now, there has not been an effective way to circumvent these underlying causes of today’s obesity epidemic.
The corpulent mass that accrues on our aging bodies can be compared to the growth of malignant tumors. This analogy goes beyond ever-increasing fat bulges and extends to how fat cells resist eradication. Like cancer, fat cells deploy multiple survival mechanisms when their existence is threatened.
So while many ways have been developed to assist people in losing weight, nothing has been shown to circumvent the natural ability of adipocytes (fat cells) to propagate and retain excess fat … until now!
OBESITY IS CAUSED BY: |
It is obesity cause number four above that is the most prevalent factor involved in age-associated weight gain. Fortunately, it is now possible to control these obesity-inducing mechanisms using a natural plant extract. |
How fat cells accumulate fat
Adipocytes (fat cells) function to store calories in the body. When energy is needed, specific command signals mobilize adipocytes to release their stored fat.
The adipocyte is the primary site for fat storage. Under the microscope, adipocytes appear bloated with triglycerides, which is the form that most fat exists in the body.9-10
Age-related weight gain occurs when adipocytes (fat cells) accumulate a large amount of triglycerides and become enlarged. Obesity is characterized at the cellular level by an increase in the number and size of adipocytes in fat tissue.11-12
Adipocytes accumulate excess triglycerides due to overeating, insufficient physical activity, hormone imbalance and other causes. These factors, however, fail to address the reason why aging individuals seem to put on fat pounds despite making great efforts to eat less, taking dietary supplements and following other practices that should in theory lead to weight loss.
Role of command signals in regulating adipocytes
Young, physically active people can consume lots of calories, often without becoming overweight. One might wonder what mechanism besides physical activity enables these healthy young bodies to limit the amount of ingested fat stored in their adipocytes.
The answer is the adipocyte command signal network that controls the storage and release of triglycerides from fat cells. These signals also regulate adipocyte proliferation.
The aging process adversely affects the adipocyte command signal network, which helps explain the difficulty maturing individuals have in controlling their weight.
The three critical adipocyte command signals
Adipocytes regulate their size and number by secreting command signals.13 One such signal is the hormone leptin, which is derived from the Greek term leptos, meaning thin.
Leptin is released by adipocytes to perform two critical functions. First it signals the brain that enough food has been ingested and shuts down appetite.13-19 It then seems to exert a process whereby triglycerides stored in adipocytes are broken down into fatty acids that can be used in energy production.20-22
The second command signal released by adipocytes is a hormone called adiponectin. This hormone is an important modulator of insulin sensitivity. Adiponectin has been shown to have anti-atherosclerotic, anti-inflammatory and anti-diabetic roles.23-28 High circulating levels of adiponectin have been shown to protect against coronary artery disease, whereas low adiponectin levels are observed in overweight individuals.25, 26, 29-32 The insulin-sensitizing effects of adiponectin represent a novel treatment target for insulin resistance, Type 2 diabetes, and obesity.26, 28-41
The third adipocyte command signal is glycerol-3-phosphate dehydrogenase. This enzyme is produced in adipocytes to help convert blood sugar into triglyceride stores in fat cells.42
The three adipocyte command signals are thus:
- Leptin
- Adiponectin
- Glycerol-3-phosphate dehydrogenase
An ideal weight loss agent would increase adiponectin, decrease glycerol-3-phosphate dehydrogenase and inhibit barriers in the aging body that block the utilization of leptin.
Discovery of a West African medicinal food
Medical discoveries often start with accidental observations. For instance, British sailors where encouraged to eat limes to prevent scurvy long before anyone even knew about vitamin C. Scurvy is the acute disease one contracts when vitamin C intake is deficient.
Anecdotal information indicated that a West African medicinal food called Irvingia gabonensis might produce some weight loss effects. A scientific analysis of various Irvingia extracts revealed that they produced a wide range of biological properties that would not only induce weight loss, but also reduce the most common risk factors involved in atherosclerosis and type 2 diabetes.5-7, 43, 46, 51, 52, 54
Small studies were conducted to identify which Irvingia extract worked best in humans. Findings from the first placebo-controlled human study showed the Irvingia extract selected caused fat loss and also markedly reduced total cholesterol (by 39%), LDL (by 45%), glucose (by 32%), and triglycerides (by 45%).6
How Irvingia extract works
Weight loss-inducing agents, be they supplements, hormones or drugs, typically function via only one mechanism. Unfortunately, adipocytes possess numerous routes to ensure their continued growth and proliferation. These survival characteristics of adipocytes explain why logical methods to promote weight loss have produced only mediocre results.
Amylase is an enzyme that converts starch to sugar in the digestive tract. There is an FDA-approved weight loss drug called Acarbose® that inhibits amylase and thereby reduces the amount of sugar absorbed into the bloodstream. White kidney bean extract does the same thing.44,46 Only moderate weight loss benefits, however, have been shown with amylase inhibitors. Irvingia is an amylase inhibitor, but this is not its primary mechanism of fat loss induction.6, 46
Adiponectin is a hormone that plays a critical role in metabolic abnormalities that are associated with Type 2 diabetes, obesity, and atherosclerosis.33, 26, 28, 34-41 Higher levels of adiponectin enhance insulin sensitivity, and enhancing insulin sensitivity is important to long-term metabolic health as we age. Adipogenic transcriptional factors involved with adiponectin are also involved in the formation of new adipocytes, fat burning and endothelial function.47-49 Irvingia increases beneficial adiponectin levels and inhibits adipocyte differentiation mediated through the suppression of adipogenic transcription factors.49
 |
| Click to enlarge |
Glycerol-3-phosphate dehydrogenase is an enzyme that facilitates the conversion of blood glucose into triglycerides that increase adipocyte size. Elevated glycerol-3-phosphate dehydrogenase might contribute to the increase of triacylglycerol synthesis in obese subjects.56 Irvingia inhibits glycerol-3-phosphate dehydrogenase, thus reducing the amount of ingested sugars that are converted to body fat.42
Leptin is a hormone secreted from adipocytes. Leptin is much more abundant in the blood of obese individuals. This may at first seem illogical since leptin functions to turn off appetite while promoting breakdown of triglycerides that bloat adipocytes. One reason obese people have higher blood levels of leptin is that C-reactive protein binds with leptin and impairs leptin transport across the blood-brain-barrier and leptin signaling at a cellular level.50
The release of C-reactive protein by adipocytes, a leptin-binding protein, neutralizes the natural adipocyte-controlling effects of leptin. Obese people have more adipocytes that secrete leptin and C-reactive protein.17, 50, 51 The result is that more leptin accumulates in the blood of obese individuals because it is not able to be picked up by leptin receptor sites on cell membranes.57 Irvingia is associated with dramatically lower levels of C-reactive protein, thereby unblocking the “leptin resistance” that causes so many weight loss programs to fail.5
Irvingia may induce fat-loss via four different mechanisms:
- It up-regulates the expression of adiponectin, thereby improving insulin sensitivity.
- It is associated with lower levels of C-reactive protein and helps restore the dual weight control effects of leptin.
- It inhibits glycerol-3-phosphate dehydrogenase, thereby reducing fatty acid formation in the body and inhibiting the amount of blood glucose that converts to fat.
- It inhibits the enzyme amylase, thus reducing the amount of ingested starches that will be absorbed as sugar.
 |
Effect of Irvingia on weight loss, blood fats and glucose
In 1990, researchers studied the effects of Irvingia on eleven human Type 2 diabetics. Compared to baseline, there were significant reductions in blood triglyceride levels (16%), total cholesterol (30%), LDL (39 %), and glucose (38%), while HDL-cholesterol levels were increased by 29% after four-week supplementation. These desirable biochemical effects were accompanied by improved clinical states.43
In 2005, researchers fed guinea pigs a high-fat diet with or without Irvingia. The guinea pigs receiving the Irvingia displayed a significant increase in beneficial HDL accompanied by a significant decrease in triglycerides and LDL. After three weeks, the Irvingia-supplemented animals lost more than 7% of their body weight; whereas the control group fed the same high-fat diet (without Irvingia) showed more than 8% increase in body weight.52
 |
In 2006, researchers studied the effect of Irvingia in rats who were artificially induced to develop diabetes. Just a single oral dose of Irvingia lowered plasma glucose two hours after treatment.46
Another study in 2006 evaluated the effects of Irvingia in slowing the intestinal absorption of glucose in healthy rats. The results showed a significant reduction in after-meal glucose blood level and lower subsequent fasting glucose scores.54
The first double-blind study in humans occurred in 2005. Twenty eight of the subjects received Irvingia while twelve were given a placebo. All subjects maintained their normal calorie intake. After 30 days, subjects taking Irvingia lost 12.3 pounds. The Irvingia group also experienced significant reductions in total cholesterol, LDL, triglycerides and an increase in HDL.6
The most significant Irvingia study
 |
Based on consistent findings showing multiple beneficial effects of Irvingia, a larger study was conducted on overweight and obese participants over a 10-week period. Participants were randomly divided in two groups, one that received Irvingia extract (150 mg twice daily), and the other was given a placebo, while maintaining the same diet and amount of physical exercise.5
Body weight and the following blood levels were measured at baseline:
- Total Cholesterol, LDL and HDL
- Fasting glucose
- Leptin
- Adiponectin
- C-reactive protein
The chart below shows the weight loss effects measured at three different times during the ten week study:5
Baseline weight |
4 weeks |
8 weeks |
10 weeks | |
| Irvingia group |
215 pounds |
207 pounds |
197 pounds |
187 pounds |
| Placebo group |
212 pounds |
210 pounds |
209 pounds |
211 pounds |
The chart above shows the Irvingia group lost 28 pounds, whereas the placebo group lost virtually no weight.
The results from the blood measurements showed equally remarkable effects after ten weeks as follows:5
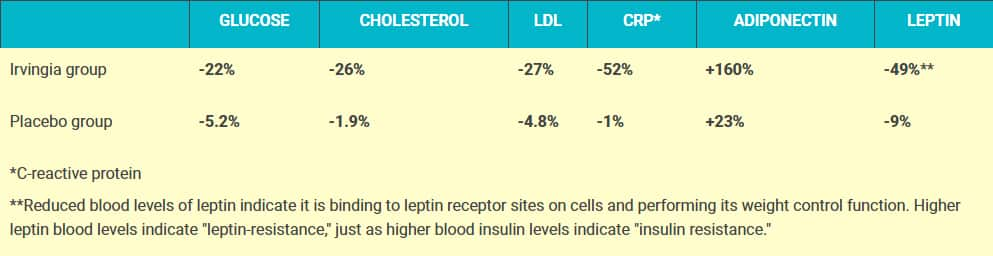 |
These remarkable blood marker changes reveal specific mechanisms responsible for the profound weight loss effects observed in subjects receiving Irvingia. These beneficial blood marker changes would also confer considerable protection against diabetes and vascular disease beyond the fat loss benefits.
When assessing body composition in these study subjects, the following changes were measured at 10 weeks:5
Waist Reduction |
Fat Loss | |
| Irvingia group |
16.2% |
18.4% |
| Placebo group |
5.0% |
5.7% |
This historic study demonstrated that Irvingia induced more weight loss in a shorter period of time than any other compound ever tested. Participants who received Irvingia had significant improvements in body composition and reductions in blood measurements of cardiovascular and diabetes risk.
The charts below show the percentage of changes seen in the Irvingia group compared to the placebo group.
 |
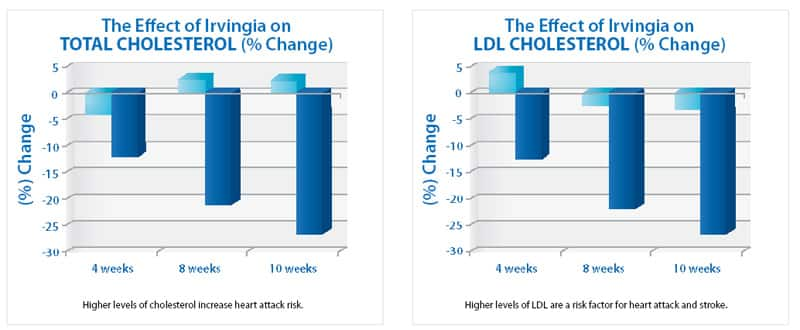 |
| Irvingia on Weight & Fasting Blood Glucose | Irvingia on Total Cholesterol & LDL Cholesterol |
 |
 |
| Irvingia on C-reactive Protein & Adiponectin | Irvingia on Leptin |
Dosage
Scientists have spent many years identifying the specific Irvingia extract that promotes the greatest amount of weight loss, while reducing blood fat (lipid) and glucose levels.
In the most significant study to date, it required only 150 mg of standardized Irvingia extract taken two times a day to produce the dramatic results, i.e. 28 pounds of weight loss in subjects taking Irvingia extract compared to less than 3 pounds of weight loss in the placebo group.
Considering the profound effect of Irvingia in sharply reducing blood glucose and cholesterol, the dose of 150 mg of Irvingia taken two times a day should not be exceeded.
Precautions
Optimal cholesterol levels range from 180 to 200 mg/dL. Cholesterol over 200 increases heart attack risk, whereas cholesterol below 150–160 mg/dL seems to increase overall mortality, probably from diseases like hemorrhagic stroke and cancer along with deficiencies of hormones that are made from cholesterol.
If you use cholesterol-lowering drugs and start taking Irvingia, have your blood tested after 30 days to make sure that your cholesterol level is not being lowered too much. If your total cholesterol drops below 160, ask your doctor to consider reducing the dose or eliminating your statin drug.
Hypoglycemics (low blood sugar) should use this product with caution as it can significantly lower blood glucose levels.
Diabetics taking medications to lower glucose levels should use this product with caution as it might cause glucose to drop too low. Diabetics are encouraged to carefully monitor their blood glucose levels, in coordination with their physician, to make sure the proper doses of anti-diabetic drug(s) are taken. If blood glucose levels drop too low, ask your doctor if the dose of anti-diabetic drug can be lowered, or the drug(s) discontinued altogether. If a diabetic experiences significant weight loss with Irvingia, their need for anti-diabetic drugs may be reduced or eliminated. Careful self measurement of blood glucose levels is crucial for all diabetics.
IRVINGIA |
| has been shown to work via multiple pathways to promote effective fat loss by such mechanisms as:
|
Summary and warning to not overeat
Endeavors to manage age-associated surplus body fat buildup have been challenging.
Just when new methods are discovered to reduce fat stores, scientists uncover additional mechanisms by which adipocytes retain excess triglycerides.
Irvingia seems to overcome the multiple escape routes that enable fat cells (adipocytes) in aging bodies to resist eradication.
Last year I wrote an article titled “Why a 100% Effective Diet Pill Would Lead to a Health Catastrophe.”55 My article stated that most people restrict their calorie intake not for health reasons but to avoid becoming too fat. I warned that if a diet pill ever emerged that did not require food restriction, most people would overeat themselves into an early grave.
It is still too early to know for sure if Irvingia will prove to be a 100% effective diet pill.
With our knowledge about the health and longevity benefits of restricting calorie intake, I beg, plead, and reiterate my point that if you find an effective method to lose weight without dieting, please continue to control calorie intake anyway in order to extend your life.
 |
In other words, if Irvingia were to work for you as well as it did for the study subjects, please do not overeat, as excess calorie intake is a leading cause of cancer, vascular disease, and accelerated aging. The good news is that by freeing up leptin to bind to hunger-control centers in the brain, most people will find their appetite is reduced when taking Irvingia, thus eabling them to effortlessly ingest fewer calories.
Note: The issue of Life Extension Magazine that members will receive in early January 2009 will feature an in-depth scientific report on obesity and the role that adipocyte modulating agents like leptin and adiponectin play in regulating body fat storage.
1. Zelissen PM, Stenlof K, Lean ME, et al. Effect of three treatment schedules of recombinant methionyl human leptin on body weight in obese adults: a randomized, placebo-controlled trial. Diabetes Obes Metab. 2005 Nov; 7(6):755-61.
2 Patel SB, Reams GP, Spear RM, Freeman RH, Villarreal D. Leptin: linking obesity, the metabolic syndrome, and cardiovascular disease. Curr Hypertens Rep. 2008 Apr;10(2):131-7.
3. Scarpace PJ, Zhang Y. Elevated leptin: consequence or cause of obesity? Front Biosci. 2007 May 1;12:3531-44. Review.
4. Enriori PJ, Evans AE, Sinnayah P, Cowley MA. Leptin resistance and obesity. Obesity. 2006 Aug;14 Suppl 5:254S-258S. Review.
5. Ngondi JL, Matsinkou R, Oben JE. The use of Irvingia gabonensis extract (IGOB131) in the management of metabolic syndrome in Cameroon. Nutrition J. 2008 (submitted).
6. Ngondi JL, Oben JE, Minka SR. The effect of Irvingia gabonensis seeds on body weight and blood lipids of obese subjects in Cameroon. Lipids Health Dis. 2005 May 25;4:12.
7. Omoruyi F, Adamson I. Digestive and hepatic enzymes in streptozotocin-induced diabetic rats fed supplements of dikanut (Irvingia gabonensis) and cellulose. Ann Nutr Metab. 1993 37(1):14-23.
8. Adamson I, Okafor C, Abu-Bakare A. A supplement of Dikanut (Irvingia gabonesis) improves treatment of type II diabetics. West Afr J Med. 1990 Apr-Jun;9(2):108-15.
9. Smith J, Al-Amri M, Dorairaj P, Sniderman A. The adipocyte life cycle hypothesis. Clin Sci (Lond). 2006 Jan;110(1):1-9.
10. Azain MJ. Role of fatty acids in adipocyte growth and development. J Anim Sci. 2004 Mar;82(3):916-24.
11. Kiess W, Petzold S, Töpfer M, Garten A, Blüher S, Kapellen T, Körner A, Kratzsch J. Adipocytes and adipose tissue.Best Pract Res Clin Endocrinol Metab. 2008 Feb;22(1):135-53.
12. Rabkin SW. Epicardial fat: properties, function and relationship to obesity.Obes Rev. 2007 May;8(3):253-61.
13. Ahima RS, Lazar MA. Adipokines and the peripheral and neural control of energy balance. Mol Endocrinol. 2008 May;22(5):1023-31.
14. Friedman JM. The function of leptin in nutrition, weight, and physiology. Nutr Rev. 2002 Oct;60(10 Pt 2):S1-14.
15. Cohen P, Zhao C, Cai X, et al. Selective deletion of leptin receptor in neurons leads to obesity. J Clin Invest. 2001 Oct;108(8):1113-21.
16. Campfield LA, Smith FJ, Guisez Y, Devos R, Burn P. Recombinant mouse OB protein: evidence for a peripheral signal linking adiposity and central neural networks. Science. 1995 Jul 28;269(5223):546-9.
17. Bray GA, York DA. Leptin and clinical medicine: a new piece in the puzzle of obesity. J Clin Endocrinol Metab. 1997 Sep;82(9):2771-6.
18. Maffei M, Halaas J, Ravussin E, et al. Leptin levels in human and rodent: measurement of plasma leptin and ob RNA in obese and weight-reduced subjects. Nat Med. 1995 Nov;1(11):1155-61.
19. Qi Y, Takahashi N, Hileman SM, et al. Adiponectin acts in the brain to decrease body weight. Nat Med. 2004 May;10(5):524-9.
20. Kim WK, Lee CY, Kang MS, et al. Effects of Leptin on Lipid Metabolism and Gene Expression of Differentiation-Associated Growth Factors and Transcription Factors during Differentiation and Maturation of 3T3-L1 Preadipocytes. Endocr J. 2008 May 23. [Epub ahead of print]
21. Tajima D, Masaki T, Hidaka S, Kakuma T, Sakata T, Yoshimatsu H. Acute central infusion of leptin modulates fatty acid mobilization by affecting lipolysis and mRNA expression for uncoupling proteins. Exp Biol Med (Maywood). 2005 Mar;230(3):200-6.
22. Frühbeck G, Gómez-Ambrosi J, Salvador J. Leptin-induced lipolysis opposes the tonic inhibition of endogenous adenosine in white adipocytes. FASEB J. 2001 Feb;15(2):333-40.
23. Pajvani UB, Du X, Combs TP, et al. Structure-function studies of the adipocyte-secreted hormone Acrp30/adiponectin. Implications for metabolic regulation and bioactivity. J Biol Chem. 2003 Mar 14;278(11):9073-85.
24. Matsuzawa Y. Adiponectin: Identification, physiology and clinical relevance in metabolic and vascular disease. Atheroscler Suppl. 2005 May;6(2):7-14.
25. Okui H, Hamasaki S, Ishida S, et al. Adiponectin is a better predictor of endothelial function of the coronary artery than HOMA-R, body mass index, immunoreactive insulin, or triglycerides. Int J Cardiol. 2008 May 7;126(1):53-61.
26. Fasshauer M, Paschke R, Stumvoll M. Adiponectin, obesity, and cardiovascular disease. Biochimie. 2004 Nov;86(11):779-84.
27. Gil-Campos M, Cañete RR, Gil A. Adiponectin, the missing link in insulin resistance and obesity. Clin Nutr. 2004 Oct;23(5):963-74.
28. Shand BI, Scott RS, Elder PA, George PM. Plasma adiponectin in overweight, nondiabetic individuals with or without insulin resistance. Diabetes Obes Metab. 2003 Sep;5(5):349-53.
29. Nakamura T, Kodama Y, Takano H, et al. Increase in circulating levels of adiponectin after treatment with statin and fibrate in patients with coronary artery disease and hyperlipidemia. Atherosclerosis. 2007 Aug;193(2):449-51.
30. Pischon T, Girman CJ, Hotamisligil GS, Rifai N, Hu FB, Rimm EB. Plasma adiponectin levels and risk of myocardial infarction in men. JAMA. 2004 Jul 7;292(1):40.
31. Han SH, Quon MJ, Kim JA, Koh KK. Adiponectin and cardiovascular disease: response to therapeutic interventions. J Am Coll Cardiol. 2007 Feb 6;49(5):531-8.
32. Kumada M, Kihara S, Sumitsuji S, et al. Association of hypoadiponectinemia with coronary artery disease in men. Arterioscler Thromb Vasc Biol. 2003 Jan 1;23(1):85-9.
33. Berger J, Moller DE. The mechanisms of action of PPARs. Annu Rev Med. 2002 53:409-435.
34. Yamauchi T, Kamon J, Waki H, et al. The fat-derived hormone adiponectin reverses insulin resistance associated with both lipoatrophy and obesity. Nat Med. 2001 7:941-946.
35. Kadowaki T, Yamauchi T. Adiponectin and adiponectin receptors. Endocr Rev. 2005 May;26(3):439-51.
36. Kershaw EE, Flier JS. Adipose tissue as an endocrine organ. J Clin Endocrinol Metab. 2004 Jun;89(6):2548-56.
37. Hotta K, Funahashi T, Bodkin NL, et al. Circulating concentrations of the adipocyte protein adiponectin are decreased in parallel with reduced insulin sensitivity during the progression to type 2 diabetes in rhesus monkeys. Diabetes. 2001 May;50(5):1126-33.
38. Arita Y, Kihara S, Ouchi N, et al. Paradoxical decrease of an adipose-specific protein, adiponectin, in obesity. Biochem Biophys Res Commun. 1999 Apr 2;257(1):79-83.
39. Ryo M, Nakamura T, Kihara S, et al. Adiponectin as a biomarker of the metabolic syndrome. Circ J. 2004 Nov;68(11):975-81.
40. Yatagai T, Nagasaka S, Taniguchi A, et al. Hypoadiponectinemia is associated with visceral fat accumulation and insulin resistance in Japanese men with type 2 diabetes mellitus. Metabolism. 2003 Oct;52(10):1274-8.
41. Yamamoto Y, Hirose H, Saito I, Nishikai K, Saruta T. Adiponectin, an adipocyte-derived protein, predicts future insulin resistance: two-year follow-up study in Japanese population. J Clin Endocrinol Metab. 2004 Jan;89(1):87-90.
42. Wise LS, Green H. Participation of one isozyme of cytosolic glycerophosphate dehydrogenase in the adipose conversion of 3T3 cells. J Biol Chem. 1979 Jan 25;254(2):273-5.
43. Adamson I, Okafor C, Abu-Bakare A. A supplement of Dikanut (Irvingia gabonesis) improves treatment of type II diabetics. West Afr J Med. 1990 Apr-Jun;9(2):108-15.
44. Udani J, Hardy M, Madsen DC. Blocking carbohydrate absorption and weight loss: a clinical trial using Phase 2 brand proprietary fractionated white bean extract. Altern Med Rev. 2004 Mar;9(1):63-9.
45. Celleno L, Tolaini MV, D’Amore A, Perricone NV, Preuss HG. A dietary supplement containing standardized Phaseolus vulgaris extract influences body composition of overweight men and women. Int J Med Sci. 2007 Jan 24;4(1):45-52.
46. Ngondi JL, Djiotsa EJ, Fossouo Z, Oben J. Hypoglycaemic effect of the methanol extract of irvingia gabonensis seeds on streptozotocin diabetic rats. Afr J Trad CAM. 2006 3:74–7.
47. Rosen ED, Walkey CJ, Puigserver P, Spiegelman BM. Transcriptional regulation of adipogenesis. Genes Dev. 2000 Jun 1;14(11):1293-307.
48. Gustafson B, Jack MM, Cushman SW, Smith U. Adiponectin gene activation by thiazolidinediones requires PPAR gamma 2, but not C/EBP alpha-evidence for differential regulation of the aP2 and adiponectin genes. Biochem Biophys Res Commun. 2003 Sep 5;308(4):933-9.
49. Oben JE, Blum K. Inhibition of OB131 Irvingia gabonensis seed extract (gabonectin™) on adipogenesis as mediated via down regulation of the PPARγ and leptin genes and up-regulation of the adiponectin gene. Lipids Health Dis. 2008. (submitted)
50. Sinha MK, Opentanova I, Ohannesian JP, et al. Evidence of free and bound leptin in human circulation. Studies in lean and obese subjects and during short-term fasting. J Clin Invest. 1996 Sep 15;98(6):1277-82.
51. Dagogo-Jack S, Fanelli C, Paramore D, Brothers J, Landt M. Plasma leptin and insulin relationships in obese and nonobese humans. Diabetes. 1996 May;45(5):695-8.
52. Ngondi JL, Makamto SC, Oben J. Irvingia gabonensis on body weight and bloods lipids in normolipidemic guinea pigs. J Food Technology. 2005;3(4): 472-474.
53. Available at: http://www.bioline.org.br/request?tc06054. Accessed: Sept. 10, 2008.
54. Ngondi JL, Fossouo E, Djiotsa EJ, Oben J. Glycaemic variations after administration of Irvingia gabonensis seeds fractions in normoglycemic rats. Afr J Trad CAM. 2006;3:94-101.
55. Available at: https://www.lifeextension.com/magazine/2008/3/ why-an-effective-diet-pill-would-lead-to-a-health-catastrophe. Accessed: Sept. 10, 2008.
56. Swierczynski J, Zabrocka L, Goyke E, Raczynska S, Adamonis W, Sledzinski Z. Enhanced glycerol 3-phosphate dehydrogenase activity in adipose tissue of obese humans. Mol Cell Biochem. 2003 Dec;254(1-2):55-9.
57. Chen K, Li F, Li J, et al. Induction of leptin resistance through direct interaction of C-reactive protein with leptin. Nat Med. 2006 Apr;12(4):425-32
Wellness
Specialists
1-800-226-2370 - This service is FREE
7:30 AM - 12 AM (ET) Mon-Fri | 9 AM - 12 AM (ET) Sat-Sun