Life Extension Magazine®
|
A unique opportunity to save countless lives and billions of dollars is being overlooked by the medical community. This technique increases blood flow to the heart, strengthens the circulation, and offers a proven way to treat heart disease in lieu of stents or bypass surgery. Enhanced external counterpulsation (EECP) is a safe, non-invasive procedure that can overcome heart disease in two ways—by passively exercising the heart to strengthen the vascular system and by targeting inflammation, the underlying culprit in damaged blood vessels that inhibits blood flow.
More than 100 studies have demonstrated its overwhelming effectiveness and unquestioned safety in improving blood flow in patients with heart disease. Some experts are calling for the EECP procedure to become first-line therapy for heart disease, long before surgery or other invasive procedures are used. Approved by the FDA for chronic stable angina, cardiogenic shock, congestive heart failure, as well as during a heart attack, EECP not only saves lives but is also considerably cheaper and safer than traditional invasive procedures such as angioplasty and coronary stents, which continue to be the mainstay of therapy. Medicare even pays for it! By improving circulation, this simple procedure prevents arteries from becoming blocked, allowing the heart to do its job more effectively. As is often the case, health care in the United States is often driven by lucrative revenues making many in the medical community reluctant to embrace alternative therapies. What you need to know
Life Extension first enlightened members to the benefits of EECP therapy in May 2003, yet most Foundation members still don’t realize this life-saving technology is available. In this article, we’ll review why your cardiologist can no longer afford to ignore the benefits of this inexpensive, life-saving procedure.
For patients with some forms of heart disease, enhanced external counterpulsation (EECP) is a non-invasive, high-tech, low-risk procedure, performed on an outpatient basis, which offers a remarkable reprieve from some of the potentially disabling symptoms of stable angina and coronary heart disease. Patients lucky enough to be offered this underused therapy may experience changes in their conditions that range from significant pain relief to renewed mobility and energy, to a rekindled libido. They may also literally gain a new lease on life, simultaneously avoiding the dangers of coronary bypass surgery while buying enough time to reverse the heart disease that brought them to this crossroads in the first place. But chances are, unless you inquire about it, you’ll never even be told this option exists. Imagine this scenario. You’ve developed troubling symptoms recently—shortness of breath, difficulty climbing stairs without resting frequently, and maybe even some pressure or pain in your chest. If you’re a man, you may have noticed a decrease in libido, or an occasional inability to sustain erection during sex. You may even break out into a sweat inexplicably from time to time. You see a physician, and after listening to your heart and lungs he may send you to see a cardiologist, who takes your history, listens to your heart again, and sends you for a battery of tests. You may be given an electrocardiogram and a chest X-ray, have some blood work drawn, and be sent for further testing, such as a stress test or an echocardiogram (EKG). Eventually, the doctor delivers the grim news, “You have coronary heart disease and you need coronary bypass surgery now.” Frightened into a near-myocardial infarction right then and there, you’re ready to agree to anything. An All-Too-Common ScenarioOr perhaps the doctor recommends balloon angioplasty, followed by insertion of a stent—a tiny metallic mesh tube that will be threaded into one (or more) of the arteries supplying blood to your heart. Once in place it will squish the sludge blocking that artery up against the artery walls, allowing blood to flow more freely again. The stent will maintain this opening—at least temporarily. Even with additional drugs, restenosis (reclosing) of the artery, is common.1 Like any educated American, you know that our medical system is the most technologically advanced that has ever existed. We don’t just bury people with heart disease, we fix them. If your drain pipes are clogged, after all, a plumber reams them out until they flow freely again. If it works for my plumbing, you reason, surely it will work for me, too.
In this all-too-common scenario, the doctor schedules time in the cardiac catheterization lab immediately. You steel yourself for an invasive procedure that has numerous risks, and costs more than your last car, but may save your life. You’ve been presented with all the options and agree with your cardiologist that balloon angioplasty followed by stent placement is the best choice of treatment. You accept that you need this procedure immediately. And so you submit to an invasive procedure that you’re convinced will improve your long-term chances of recovery. This is the best option for treatment, bar none, and thank goodness you’re living in a country where such procedures are performed so routinely. But is it really the best option? What if there were another treatment option that could achieve some of the potential benefits of angioplasty, and maybe more, without invasive surgery? Too Good to be True?Debra Braverman, MD, is one of the country’s leading experts on enhanced external counterpulsation (EECP). She is also one of its most enthusiastic proponents. She runs the largest EECP facility in the nation, the Braverman EECP Heart Centers, affiliated with Albert Einstein Healthcare Network, in Philadelphia, Pennsylvania. “The first time I heard about it, I thought it sounds too good to be true,” says Dr. Braverman (who, incidentally, is not related to Dr. Eric Braverman). But that was years ago. Now, she’s a firm believer in this deceptively simple therapy for a deadly disease. “I was amazed by the science behind it and the simplicity of the technique. In our culture, we tend to think the higher-tech, the better, but the results with this technique are phenomenal.”
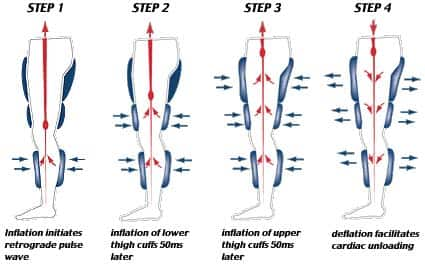
This simple procedure is done as an outpatient therapy that patients ordinarily receive in a series of sessions, lasting roughly one hour per day, for up to seven weeks, for a total of 35 sessions. While the patient lies on a special bed, inflatable cuffs, much like blood pressure-monitoring cuffs, are wrapped around the lower and upper legs. An electrocardiogram monitors the patient’s heartbeat, and a computer coordinates a cycle of rapid inflations and deflations of the cuffs in rhythm with the patient’s heartbeat. Cuff contractions occur during the resting phase of the patient’s pulse. Forcing blood back into the heart, they effectively take some of the workload off the heart. Patients ordinarily report finding the experience relaxing, akin to deep-tissue massage; within weeks, or even days, they usually report feeling more energetic and having a greater tolerance for exercise, in addition to relief from angina pain, according to Dr. Braverman. She notes that more than 100 articles about EECP have been published in the medical literature. Numerous clinical trials have shown time and again that EECP is effective at relieving pain and other symptoms of angina in patients with stable angina. It has also proven effective at improving symptoms of heart failure, reducing patient reliance on medications, and improving exercise tolerance, erectile function, and quality of life. In other countries, it has been used to successfully treat peripheral vascular disease, restless leg syndrome, peripheral neuropathy, and to improve wound care.2-4 Cardiovascular benefits have been shown to last for up to five years. What’s more, in comparison with riskier, more expensive, and far more common interventional procedures such as angioplasty and coronary bypass, studies have shown that EECP is as good or better at alleviating symptoms, reducing morbidity, and improving quality of life.4-21 In her book, Heal Your Heart with EECP—The First Comprehensive Guide to Enhanced External Counterpulsation, Dr. Braverman describes clinical trials that showed coronary heart disease patients who received EECP, rather than angioplasty, were less likely to undergo repeat treatment at one- and five-year follow-up than patients treated with angioplasty.3,22-24 Other data analysis found that within five years of initial treatment, patients treated with coronary bypass, angioplasty, or EECP all experienced similar subsequent mortality and heart attack rates, although the rate of deaths within five years was slightly lower for both EECP and bypass surgery than for angioplasty.3,22,24
Forging New Pathways—Repairing the Heart’s Blood SupplyRegarded as a form of physical therapy, EECP stands in sharp contrast to the other, far more common approaches to angina; namely invasive interventions such as cardiac catheterization, angioplasty, stent placement, and coronary artery bypass surgery. “This is a systemic disease,” notes Dr. Braverman. “Invasive procedures don’t address the underlying heart disease.” Atherosclerotic plaques can prevent blood flow to the heart muscle, resulting in oxygen starvation of the cardiac muscle tissue. These clinical manifestations are often characterized by the pain of angina and some loss of cardiac function. But these blockages “often become irrelevant,” says Dr. Braverman. “EECP improves blood flow by improving blood vessel function as a whole…New pathways form.”
This phenomenon, known as coronary collateral angiogenesis, is well documented. In recent years, scientists have devoted increasing time and resources to the quest for therapies designed to encourage this process.25-27 Miami-based preventive cardiologist, Michael D. Ozner, MD, FACC, FAHA, characterizes the development of these remarkable new vessels as “natural heart bypass.” He advocates medical over surgical therapies, noting that it is possible to live with blockages, while reversing the underlying atherosclerosis, through dramatic lifestyle changes, such as adherence to a Mediterranean-type diet and exercise. This inherent ability of the body to recruit existing small vessels and transform them into alternate routes for coronary circulation—natural bypasses around arterial blockages—may be attributed to increased production of stem cells from which endothelial cells are formed called endothelial “progenitor” cells. And research shows that these progenitor cells increase significantly in response to exercise. This increase is also tied to improved endothelial function.28-31 The endothelium (the tissue lining blood vessel walls) plays a central role in the development of atherosclerosis; it is here in the endothelium that the process begins. Unless reversed with diet, exercise, and/or drug therapy, atherosclerosis ordinarily culminates in cardiovascular disease. The ability to improve endothelial function by exercise, mediated by increased production of endothelial progenitor cells, is partly responsible for the cardiovascular health benefits of exercise. Not coincidentally, EECP simulates intensive exercise.
“EECP absolutely mimics exercise,” says Dr. Braverman. “The machine is exercising for them in a sense. It truly recreates the circulatory benefits of exercise.” This exercise-like benefit is believed to derive from hemodynamic shear stress effects created by EECP. This refers to the phenomenon in which fast-moving blood particles interact with the blood vessel walls. This mechanical phenomenon, specifically as experienced during EECP, has recently been linked to suppression of inflammation in patients with angina and coronary artery disease.32 By forcing blood through relaxed blood vessels, shear stresses on the vascular walls may also stimulate the production of endothelial progenitor cells,33 just as exercise does. In any event, this mechanical effect, which is induced by exercise or EECP, has been shown to stimulate collateral vessels in the coronary circulation.34 In addition, some other studies have shown that EECP is associated with increased levels of the crucial vasodilator nitric oxide.35 Dr. Braverman says, “There is considerable evidence that numerous conditions—including hypertension, obesity, high cholesterol, diabetes, heart failure, atherosclerosis, aging, and vascular injury—are associated with endothelial dysfunction and reduced nitric oxide levels. Anything that increases nitric oxide will have a long-term beneficial effect on heart disease and angina, and will improve the circulation in your entire body.” In addition, EECP reduces plasma levels of brain natriuretic peptide (a marker associated with heart failure).36 Studies in animals also show that EECP helps alleviate processes associated with atherogenesis, including decreasing hypercholesterolemia-induced endothelial damage and arresting vascular smooth muscle cell proliferation and migration.37 A Bridge to Self-Sustaining TherapyAccording to Dr. Braverman, “EECP truly recreates the circulatory benefits of exercise…It’s a bridge for many of our patients. It enables these people to overcome their symptoms and then pursue their own exercise program.” This is crucial, she points out, since “some can barely walk at first.” She recognizes that the gains made through EECP must be leveraged by the patient once the treatment cycle is complete. The ultimate solution for heart disease, she notes “has got to be a lifestyle solution.” The procedure is not some sort of glorified crutch for her patients. “No patient is doing EECP and then going home to sit on the couch. It enables them to pursue an active lifestyle. These patients want to enjoy an active lifestyle,” she says, and EECP provides that second chance to make permanent changes for the better. “What we’re trying to do is slow, if not halt, heart disease. EECP allows the body to heal itself; it’s efficacious in turning around the progression of heart disease,” she says.
Ariel Soffer, MD, FACC, is a prominent Hollywood, Florida-based cardiologist who notes that EECP was approved by the FDA for the treatment of coronary artery disease and angina in 1995. In 2002, EECP was also approved for the treatment of congestive heart failure. Over the years he has treated “hundreds, maybe thousands” of patients with EECP. “They come to us in droves,” he notes. “We have [an EECP treatment] room running every day.” His patients who receive EECP therapy “are some of our happiest patients,” he says. “They’re also some of the most vocal advocates for EECP.” Dr. Soffer, who is the official preventive cardiologist for the National Hockey League’s Florida Panthers, was among the first doctors in the area to utilize EECP, which is often viewed as physical therapy, or rehabilitation. Not all patients are candidates for EECP therapy. Some patients with aortic aneurysm, for instance, or certain patients on high-dose Coumadin® therapy may be excluded. Dr. Braverman notes that presence of aortic aneurysm is not necessarily cause for exclusion from EECP therapy in her practice. She says she accepts patients with abdominal aortic aneurysm, as long as it is less than 5 cm in diameter. Similarly, patients on Coumadin® therapy may not necessarily be excluded. “[It] really depends on how stable they are on the medication,” she says, “I have treated many patients with fairly high levels without any bleeding or bruising complications.” Dr. Soffer notes, “It’s applicable for most patients. It’s amazing that we don’t do it more often in this country.” Rather, American doctors, “tend to use more invasive treatments. We have a ‘cut it out’ mentality,” he says. But EECP achieves some remarkable outcomes, without invasive treatment. “It’s really opened our eyes to the ability of the heart to revascularize itself,” he says. “We’ve catheterized patients [in the cardiac catheterization lab] and found better circulation after EECP. After a course of EECP treatment, patients experience elevated exercise capacity, elevated mood, and increased sexual capacity. “There are significant improvements,” he says, noting that most results are obtained within the first six weeks of therapy. “EECP should be discussed with the patient as an alternative, versus bypass or stent,” says Dr. Soffer. “I really, truly believe the patient needs to be the captain of their own ship…In the US we are more invasive in our treatments, but I think EECP is being underused.” While the cardiology community has been somewhat slow to embrace this safe, effective, non-invasive treatment, Dr. Soffer believes that it will gradually gain acceptance as an alternative or adjuvant treatment. “As people begin to look more and more at integrative and alternative therapies, this will begin to become more popular, particularly as the cost of the machines comes down.” The bottom line is difficult to argue with…“It’s proven to increase blood flow” he notes. Dr. Braverman is also hopeful that EECP use will increase, but she is somewhat skeptical. She is frustrated by physicians’ unwillingness to share information with their patients regarding this safe alternative to invasive procedures, such as bypass surgery and angioplasty. And she seems unconvinced that the cost of EECP machinery is a prohibitive factor. “The equipment is really not that expensive versus other cardiology equipment,” she says. “It’s not as lucrative as more invasive procedures, reimbursement is low…It’s a tragedy that doctors don’t even mention or offer it,” she says. “Billions of dollars are being spent on heart disease. A lot of medicine is driven by money and not by science, and that’s got to change.” The onus is on physicians to practice full disclosure. “The physician is bound to tell the patient all options, to have an open dialogue with patients. Those who don’t include EECP are withholding information. There’s no justification for it.” Ruefully, she notes that only a fraction of the patients who could benefit from this treatment are sent to her by cardiologists. But those same cardiologists are quick to send their own family members, when they have heart disease. “There’s nothing negative to say about this treatment,” she concludes. “There are amazing clinical benefits with this technique.” If you have any questions on the scientific content of this article, please call a Life Extension Wellness Specialist at 1-800-226-2370. More Information Regarding EECPIn the Northeast, contact: In Florida, contact: |
|||||||||||||
| References | |||||||||||||
|
1. Zakliczynski M, Lekston A, Osuch M, et al. Comparison of long-term results of drug-eluting stent and bare metal stent implantation in heart transplant recipients with coronary artery disease. Transplant Proc. 2007 Nov;39(9):2859-61. 2. Rajaram SS, Shanahan J, Ash C, Walters AS, Weisfogel G. Enhanced external counter pulsation (EECP) as a novel treatment for restless legs syndrome (RLS): a preliminary test of the vascular neurologic hypothesis for RLS. Sleep Med. 2005 Mar;6(2):101-6. 3. Braverman D. Heal Your Heart with EECP—The First Comprehensive Guide to Enhanced External Counterpulsation. Berkeley, CA:Celestial Arts;2005. 4. Sajja V, Dod H, Beto R, et al. An analysis of the efficacy and safety of enhanced external counterpulsation at West Virginia University Hospitals. WV Med J. 2007 May;103(3):10-2. 5. Manchanda A, Soran O. Enhanced external counterpulsation and future directions: step beyond medical management for patients with angina and heart failure. J Am Coll Cardiol. 2007 Oct 16;50(16):1523-31. 6. Arora RR, Shah AG. The role of enhanced external counterpulsation in the treatment of angina and heart failure. Can J Cardiol. 2007 Aug;23(10):779-81. 7. Soran O. A new treatment modality in heart failure enhanced external counterpulsation (EECP). Cardiol Rev. 2004 Jan;12(1):15-20. 8. Yavari M, Montazeri HR. Effects of enhanced external counterpulsation on anginal symptoms and improvements in objective measures of myocardial ischaemia. Cardiovasc J Afr. 2007 May;18(3):154-6. 9. Soran O, Kennard ED, Kfoury AG, Kelsey SF. Two-year clinical outcomes after enhanced external counterpulsation (EECP) therapy in patients with refractory angina pectoris and left ventricular dysfunction (report from The International EECP Patient Registry). Am J Cardiol. 2006 Jan 1;97(1):17-20. 10. Pettersson T, Bondesson S, Cojocaru D, et al. One year follow-up of patients with refractory angina pectoris treated with enhanced external counterpulsation. BMC Cardiovasc Disord. 2006;628. 11. Zhang Y, He X, Chen X, et al. Enhanced external counterpulsation inhibits intimal hyperplasia by modifying shear stress responsive gene expression in hypercholesterolemic pigs. Circulation. 2007 Jul 31;116(5):526-34. 12. Soran O, Kennard ED, Bart BA, Kelsey SF. Impact of external counterpulsation treatment on emergency department visits and hospitalizations in refractory angina patients with left ventricular dysfunction. Congest Heart Fail. 2007 Jan;13(1):36-40. 13. Abbottsmith CW, Chung ES, Varricchione T, et al. Enhanced external counterpulsation improves exercise duration and peak oxygen consumption in older patients with heart failure: a subgroup analysis of the PEECH trial. Congest Heart Fail. 2006 Nov;12(6):307-11. 14. Cleland JG, Coletta AP, Freemantle N, et al. Clinical trials update from the American College of Cardiology meeting: CARE-HF and the remission of heart failure, Women’s Health Study, TNT, COMPASS-HF, VERITAS, CANPAP, PEECH and PREMIER. Eur J Heart Fail. 2005 Aug;7(5):931-6. 15. Feldman AM, Silver MA, Francis GS, et al. Enhanced external counterpulsation improves exercise tolerance in patients with chronic heart failure. J Am Coll Cardiol. 2006 Sep 19;48(6):1198-205. 16. Arora RR, Bergmann S. Effects of enhanced external counterpulsation (EECP) on myocardial perfusion. Am J Ther. 2007 Nov;14(6):519-23. 17. Shea ML, Conti CR, Arora RR. An update on enhanced external counterpulsation. Clin Cardiol. 2005 Mar;28(3):115-8. 18. Sinvhal RM, Gowda RM, Khan IA. Enhanced external counterpulsation for refractory angina pectoris. Heart. 2003 Aug;89(8):830-3. 19. DeMaria AN. A historical overview of enhanced external counterpulsation. Clin Cardiol. 2002 Dec;25(12 Suppl 2):II3-5. 20. Arora RR, Chou TM, Jain D, et al. The multicenter study of enhanced external counterpulsation (MUST-EECP): effect of EECP on exercise-induced myocardial ischemia and anginal episodes.J Am Coll Cardiol. 1999 Jun;33(7):1833-40. 21. Lawson WE, Hui JC, Lang G. Treatment benefit in the enhanced external counterpulsation consortium. Cardiology. 2000;94(1):31-5. 22. Lawson WE, Hui JC, Cohn PF. Long-term prognosis of patients with angina treated with enhanced external counterpulsation: five-year follow-up study. Clin Cardiol. 2000 Apr;23(4):254-8. 23. Holubkov R, Kennard ED, Foris JM, et al. Comparison of patients undergoing enhanced external counterpulsation and percutaneous coronary intervention for stable angina pectoris. Am J Cardiol. 2002 May 15;89(10):1182-6. 24. BARI Investigators. Comparison of coronary bypass surgery with angioplasty in patients with multivessel disease. The Bypass Angioplasty Revascularization Investigation (BARI) Investigators. N Engl J Med. 1996 Jul 25;335(4):217-25. 25. Matsuo Y, Imanishi T, Hayashi Y, et al. The effect of endothelial progenitor cells on the development of collateral formation in patients with coronary artery disease. Intern Med. 2008;47(3):127-34. 26. Vartanian SM, Sarkar R. Therapeutic angiogenesis. Vasc Endovascular Surg. 2007 Jun;41(3):173-85. 27. Springer ML. A balancing act: therapeutic approaches for the modulation of angiogenesis. Curr Opin Investig Drugs. 2006 Mar;7(3):243-50. 28. Van Craenenbroeck EM, Vrints CJ, Haine SE, et al. A maximal exercise bout increases the number of circulating CD34+/KDR+ endothelial progenitor cells in healthy subjects. Relation with lipid profile. J Appl Physiol. 2008 Jan 24. 29. Sarto P, Balducci E, Balconi G, et al. Effects of exercise training on endothelial progenitor cells in patients with chronic heart failure. J Card Fail. 2007 Nov;13(9):701-8. 30. Miller-Kasprzak E, Jagodzinski PP. Endothelial progenitor cells as a new agent contributing to vascular repair. Arch Immunol Ther Exp.(Warsz.). 2007 Jul;55(4):247-59. 31. Boos CJ, Blann AD, Lip GY. Assessment of endothelial damage/dysfunction: a focus on circulating endothelial cells. Methods Mol Med. 2007;139:211-24. 32. Casey DP, Conti CR, Nichols WW, et al. Effect of enhanced external counterpulsation on inflammatory cytokines and adhesion molecules in patients with angina pectoris and angiographic coronary artery disease. Am J Cardiol. 2008 Feb 1;101(3):300-2. 33. Available at: http://jap.physiology.org/cgi/reprint/00232.2003v1.pdf. Accessed March 12, 2008. 34. Bondke A, Buschmann IR, Bode C, Buschmann EE. Inducing collaterals in due time. Arteriogenesis as a preventive principle. Hamostaseologie. 2007 Dec;27(5):363-72. 35. Masuda D, Nohara R, Hirai T, et al. Enhanced external counterpulsation improved myocardial perfusion and coronary flow reserve in patients with chronic stable angina; evaluation by(13)N-ammonia positron emission tomography. Eur Heart J. 2001 Aug;22(16):1451-8. 36. Urano H, Ikeda H, Ueno T, Matsumoto T, Murohara T, Imaizumi T. Enhanced external counterpulsation improves exercise tolerance, reduces exercise-induced myocardial ischemia and improves left ventricular diastolic filling in patients with coronary artery disease. J Am Coll Cardiol. 2001 Jan;37(1):93-9. 37. Zhang Y, He X, Chen X, et al. Enhanced external counterpulsation inhibits intimal hyperplasia by modifying shear stress responsive gene expression in hypercholesterolemic pigs. Circulation. 2007 Jul 31;116(5):526-34. 38. Conti CR. Current Nonpharmacologic Management of Coronary Artery Disease: Focus on External Counterpulsation. Curr Treat Options Cardiovasc Med. 2005 May;7(1):81-6. 39. Michaels AD, McCullough PA, Soran OZ, et al. Primer: practical approach to the selection of patients for and application of EECP. Nat Clin Pract Cardiovasc Med. 2006 Nov;3(11):623-32. |






Wellness
Specialists
1-800-226-2370 - This service is FREE
7:30 AM - 12 AM (ET) Mon-Fri | 9 AM - 12 AM (ET) Sat-Sun