Life Extension Magazine®
Twenty four years ago, the Life Extension Foundation introduced coenzyme Q10 to the United States. Back then, it was sold in Japan as a prescription drug to treat heart disease. Life Extension, however, provided persuasive evidence that CoQ10 could help protect against a host of age-related disorders. Based on a large volume of favorable research, CoQ10 has become one of today’s most popular dietary supplements. In recent years, new delivery systems have been developed that transport more CoQ10 into the bloodstream than original versions. Providing greater quantities of CoQ10 to the body is of particular importance, since scientific studies show that higher CoQ10 blood levels produce superior benefits. In what may be the most significant breakthrough in the history of the dietary supplement industry, Japan’s largest CoQ10 producer has discovered a way to deliver the highest concentrations of the most biologically active form of coenzyme Q10 to the bloodstream. As you will read in this article, this improved form of CoQ10 not only absorbs up to eight times better, but also has demonstrated unprecedented anti-aging effects compared to placebo and compared to the coenzyme Q10 you are using now. Unlike outrageously priced prescription drugs, this new form of CoQ10 enables consumers to obtain more activated coenzyme Q10 in their bodies at a far lower cost. Based on the findings you are about to read, this novel CoQ10 compound (ubiquinol) could revolutionize how a number of age-related disorders are both prevented and treated. Scientists long ago discovered that orally ingesting the ubiquinone form of coenzyme Q10 produced beneficial effects on the heart,1-19 brain,1,20-24 kidneys,25-27 and other tissues.1,5,28-38 What the lay literature did not discuss was the fact that in order for the ubiquinone form of CoQ10 to be properly utilized, it first must be reduced in the body to its active metabolite known as ubiquinol. While most ubiquinone is naturally reduced to ubiquinol, the optimal way to supplement with CoQ10 would be to ingest it in its ready-to-use ubiquinol form. Since ubiquinol is highly unstable, it has been extremely difficult (until now) to make it available as a dietary supplement. After years of painstaking research, Japan’s largest producer of coenzyme Q10 has developed a patented method to stabilize ubiquinol so that it can be swallowed in a capsule for utilization by cells throughout the body.39 The ramifications of widespread use of this novel form of CoQ10 are profound. For the first time, it may be possible to achieve the sustained high blood levels of biologically active ubiquinol CoQ10 needed to delay certain manifestations of aging and its related disorders. Sharply Higher Absorption LevelsEven with today’s enhanced delivery systems, achieving optimal blood levels of CoQ10 can be challenging. Those suffering from disorders that require higher blood levels have had to consume relatively large doses of CoQ10. Ideal blood levels for those afflicted with neurological disorders (such as Parkinson’s disease) or congestive heart failure are considered to be greater than 3.5 micrograms per milliliter (mcg/mL).43 When CoQ10 is ingested in its reduced form as ubiquinol, higher blood CoQ10 levels can be achieved using smaller milligram doses. In assimilation studies on rats, oral feeding of ubiquinol CoQ10 was shown to increase blood levels more than twice as high as conventional CoQ10 (ubiquinone).44,45 Human assimilation studies are even more impressive.
As shown in Figure 1, a recent human trial showed that supplementing with just 150 mg per day of ubiquinol resulted in CoQ10 blood levels of 3.84 mcg/mL. In study subjects who took 300 mg per day of ubiquinol, blood CoQ10 levels reached 7.28 mcg/mL. This study showed that it took only four weeks to achieve these desirable high levels.46 To put these blood levels in perspective, scientists have conducted human clinical trials using very high doses of conventional CoQ10 in enhanced delivery systems. As shown in the chart above (Figure 1), one clinical study used 1200 mg per day of ubiquinone CoQ10 to achieve blood concentrations of 3.96 mcg/mL. Based on recently published absorption studies, just 150 mg per day of ubiquinol would provide virtually the same high CoQ10 blood levels as 1200 mg of enhanced-delivery ubiquinone CoQ10.46,47
As indicated in Figure 1, another study used 2400 mg per day of conventional CoQ10 to reach blood levels of 7.25 mcg/mL. Just 300 mg per day of ubiquinol was shown to provide about the same amount (7.28 mcg/mL) of CoQ10 to the blood at four weeks.46,48 A review of published studies on human subjects reveals that it requires very high doses of conventional CoQ10 to achieve the same levels attainable with modest amounts of ubiquinol CoQ10.46-50 Figure 1 clearly shows how little ubiquinol is needed to provide the same blood (plasma) levels that are achieved in response to far greater amounts of ubiquinone. This chart (Figure 1) reveals that it takes eight times more ubiquinone to increase CoQ10 blood levels to what can be achieved with much lower doses of ubiquinol. Side-by-Side Comparison of Ubiquinol and UbiquinoneIn a side-by-side single-dose human study, ubiquinol absorption was compared directly to conventional CoQ10 (ubiquinone) using the same delivery system. Subjects were given either 100 mg of ubiquinol or 100 mg of ubiquinone. To further validate the study, the subjects were crossed over, so that every participant was tested after receiving ubiquinol and later ubiquinone, and vice versa. As shown in Figure 2 (next page), the findings showed that in aged test subjects, ubiquinol absorption was 60% greater in this single-dose side-by-side comparison.51 While single-dose oral studies have some limited value, the true picture of bioavailability occurs after people have ingested CoQ10 supplements for about four weeks. In these longer-term studies, the superior absorption of ubiquinol is most pronounced. Ubiquinol Maintains Higher Blood Levels LongerAnimal and human studies clearly show that ubiquinol is much better absorbed than ubiquinone. What may be even more important is how long ubiquinol CoQ10 remains in the body compared to ubiquinone. In a study of aged rats, equal amounts of ubiquinol or ubiquinone were orally administered to evaluate how long ubiquinol would remain at increased levels in the blood. The importance of this data is that it might help explain why ubiquinol exhibits superior biological effects compared to ubiquinone.
The results of this study showed that ubiquinol ingestion caused a greater than 90% increase in blood ubiquinol levels and that this elevated level persisted for the entire eight-hour duration of the study. In response to ingestion of an equal amount of ubiquinone, blood ubiquinol levels never even reached 90% of baseline.52 This study also measured ubiquinol levels in micrograms per milliliter (mcg/mL) of blood. As you may recall, humans with certain disorders achieve optimal benefits when CoQ10 blood levels exceed 3.5 mcg/mL. In response to a modest amount of ubiquinol supplementation (the equivalent of 100 mg per day in humans), blood CoQ10 levels peaked at 6.0 (mcg/mL) and dropped to 4.5 after eight hours, as shown in Figure 3 (next page). In the group receiving an equal amount of ubiquinone, peak blood levels increased to only 2.1 (mcg/mL) and declined to 1.2 eight hours later. In this particular study, ubiquinol was present in the blood at a 3.75-fold greater concentration after eight hours compared to ubiquinone.52 | ||||||



Retarding the Aging ProcessIf all that ubiquinol did was assimilate so much better than ubiquinone, this alone would make the ubiquinol form of CoQ10 the preferred choice. What has scientists most excited, however, are the superior anti-aging effects demonstrated by the ubiquinol form of CoQ10 as compared to ubiquinone.
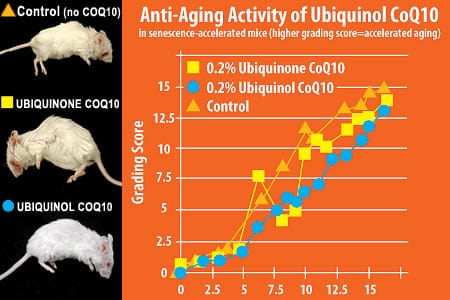
Aging humans suffer a precipitous decline in coenzyme Q10 synthesis that correlates with increased risks of multiple degenerative diseases.23,53-73 Gerontologists have long theorized that if one could maintain youthful mitochondrial energy levels, many deleterious effects of aging could be postponed. CoQ10 is a critical factor involved in healthy mitochondrial energy production. To ascertain the age-retarding effects of ubiquinol, scientists conducted a meticulous study of senescence-accelerated mice.74 One reason this mouse model is used is that it enables researchers to quickly identify compounds that may slow aging. Senescence-accelerated mice grow normally, but show early signs of aging, including reduced physical activity, loss of hair glossiness, coarse skin, hair loss, ocular lesions, and curvature of the spine. In this study, the senescence-accelerated mice were divided into three groups. Starting at two months of age, the first group continued to receive standard lab chow, while the second group’s lab chow was fortified with conventional (ubiquinone) CoQ10, and the third group’s lab chow was fortified with ubiquinol CoQ10.74 A grading score developed by the Council for Senescence Accelerated Mouse Research was used to evaluate the aging rate of the three groups of mice. A higher grading score means that biological aging is occurring faster. At three months of age, the grading score was about 0.0 for all three groups.74 As would be expected, the aging rate spiked sharply higher in the control group (not receiving any CoQ10) starting around three months of age. Mice receiving ubiquinol or ubiquinone CoQ10 showed a slower rate of aging after three months compared to the placebo group, as shown in Figure 4 (next page).74 When middle age set in (at about nine months of age), the placebo group grading score spiked up to 10.0, whereas the grading score of the groups receiving ubiquinol or ubiquinone increased to only 5.5. This translates into a 45% slower rate of aging for mice receiving ubiquinol or ubiquinone compared to placebo.74 So at nine months, it is clear that either form of CoQ10 (ubiquinol or ubiquinone) markedly slowed measurements of aging. At 10 months of age, however an incredible divergence was observed. As shown in Figure 4, the placebo group’s grading score spiked to 12, the ubiquinone group score reached 9.9, whereas the ubiquinol group score only increased to 5.9. Therefore, at a point that translates into late middle age, mice receiving ubiquinol aged 51% slower than placebo and 40% slower than the group receiving the ubiquinone form of CoQ10.74
At 12 months of age, the difference in the groups was so remarkable that the researchers decided to take photos of the mice in each group. As can be seen by the photos on the next page, a mouse receiving ubiquinol appears to be perfectly healthy, whereas a mouse receiving ubiquinone has suffered noticeable degenerative changes. The mouse receiving neither form of CoQ10 looks absolutely ghastly. As can be seen in Figure 4, at 12 months, there is relatively little difference between the placebo and ubiquinone groups in grading scores, whereas the group receiving ubiquinol shows a 22% slower rate of aging. The most startling data this chart shows, however, is that mice receiving ubiquinol dramatically slowed the rate at which age-induced degenerative changes occurred in mid-life and to a lesser degree in later life. Video Footage of 12-Month-Old MiceThe still pictures of 12-month-old mice that received ubiquinol, ubiquinone, or the control (placebo) speak for themselves. What is even more impressive is video footage comparing the different groups of mice. A video shows that in response to no supplemental CoQ10, the mouse is essentially immobile and unresponsive, exhibiting lesions in and around the eye, with spinal and limb deformities as well as a patchy, discolored coat. Many of these pathological events seen in mice not supplemented with CoQ10 are classic signs of degenerative aging suffered by elderly humans. The 12-month-old mouse supplemented with ubiquinol, on the other hand, is shown to be alert, responsive, and energetic, with no physical lesions or deformities and a glossy coat resembling that of a young, healthy mouse. Anti-Fatigue Effects of Ubiquinol in Aged RatsA universal pathological effect inflicted by aging on living organisms is mitochondrial energy depletion that manifests outwardly as fatigue. The primary mechanism by which CoQ10 protects against age-related degeneration is helping to maintain mitochondrial energy output.3
To compare the anti-fatigue effects of the ubiquinol and ubiquinone forms of CoQ10, scientists took a group of aged rats and measured how long they could run on a treadmill. In this crossover study, the control group receiving no CoQ10 showed a slight decline in treadmill running time, whereas running times increased 60% in the group receiving ubiquinone and an astounding 150% in the group receiving the ubiquinol form of CoQ10, as shown in Figure 5 (next page).75 Ubiquinol Levels Lower in Disease StatesAs humans age, there is a sharp reduction in coenzyme Q10 synthesis, with a corresponding reduction in blood ubiquinol levels. Figure 6 shows the reductions in various coenzyme Q10 tissue levels that occur with normal aging. In examining humans suffering from various pathological conditions, blood ubiquinol levels are uniformly lower.53-73 In those with diabetes, ubiquinol levels have been shown to be 74% lower than in control subjects.76 Ubiquinol decreases of 6.5% to 12.5% have been observed in those with hepatitis, liver cancer, and amyotrophic lateral sclerosis (Lou Gehrig’s disease).59-61,69 Ubiquinol’s Effect on Mitochondrial FunctionIn healthy human blood, more than 90% of coenzyme Q10 exists in its reduced ubiquinol form. An analysis of published research indicates that ubiquinol is the form of CoQ10 that most effectively suppresses free radicals and increases mitochondrial energy output.54,57,77-81 Only ubiquinol effectively scavenges lipid peroxyl radicals and prevents chain-reaction-causing oxidative damage to polyunsaturatedfatty acids of biological membranes. Ubiquinol forms an important first line of antioxidant defense in atherogenic lipoproteins such as low-density lipoprotein (LDL), and is capable of regenerating alpha-tocopherol vitamin E.54,78,79 Supplementation with the ubiquinol form of CoQ10 not only elevates blood levels of ubiquinol, but also increases the ratio of ubiquinol to total CoQ10 concentration. For example, when ubiquinol is supplemented, the ubiquinol to total CoQ10 ratio increases to 96-98.5%, compared to approximately 80-85% when ubiquinone is supplemented. Moreover, the ratio remained unchanged during administration of ubiquinone.80,81 An increase in the ratio of ubiquinol in blood, by even small percentages, may indeed have profound implications. With enzymes, a boost of as little as 3-5% can translate into powerful biological effects. Ubiquinol supplementation results in an impressive 12% increase in the ubiquinol to total CoQ10 ratio. The term “hydrophilic” means readily absorbable or dissolvable in water. Ubiquinol is the more hydrophilic form of CoQ10, which has been shown to be more stable in lipid bilayers of the cell and therefore could be very well dispersed in the mitochondria.82
Ubiquinol’s greater hydrophilic properties probably enable it to be taken up better by cells, which might result in specifically targeting the mitochondria within cells.83 In other words, since ubiquinol is more hydrophilic (that is, less capable of dissolving in fats), it would theoretically tend to be less retained in cell membranes, while achieving more significant intracellular concentrations.84 This may offer a plausible mechanism whereby ubiquinol might accumulate more effectively within mitochondria than exogenous ubiquinone, thereby exerting a greater contribution to mitochondrial energy production. Scientists are still seeking to identify the exact mechanisms by which ubiquinol so effectively enhances mitochondrial function. The ability of ubiquinol to remain at constantly higher levels in the bloodstream is one likely reason why it has demonstrated such remarkable anti-aging effects compared to ubiquinone. What is the Optimal Human Dose of Ubiquinol?Healthy people seeking to maintain more youthful coenzyme Q10 blood levels usually supplement with around 100 mg of conventional CoQ10 (ubiquinone) daily. Based on side-by-side comparative research, if these individuals were to switch to 100 mg of ubiquinol instead, they would enjoy a significant increase of CoQ10 in the blood. This alone makes ubiquinol the logical choice. Those seeking to replicate the incredible anti-aging findings of the study performed on senescence-accelerated mice should consider supplementing with 200-300 mg of ubiquinol a day. These higher doses have produced the most remarkable benefits of ubiquinol CoQ10 compared to ubiquinone CoQ10. In other words, at a dose of 100 mg per day, the benefit of ubiquinol over ubiquinone is only about 1.5-fold, whereas at higher doses, bioavailability increases up to a remarkable 8-fold.
The reason for this phenomenon is that once one exceeds 100 mg using conventional ubiquinone, the linear increase in CoQ10 blood levels slows. This is probably due to absorption saturation limitations inherent to this form of CoQ10. When doses of 150-300 mg of ubiquinol are ingested, there is an exponential increase in blood CoQ10 levels. Not only is there a greater initial spike, but there is also a greater sustained level of blood CoQ10 over an eight-hour period. Based on the totality of published research about coenzyme Q10, it would appear desirable for adults over the age of 30 to seek a minimum sustained blood level of more than 3 mcg/mL of blood. This level could be achieved by supplementing with two to three 50-mg ubiquinol capsules daily, depending on one’s age, daily calorie intake, and body weight. Ideally, one would take ubiquinol in two divided doses to achieve consistent blood levels throughout the day. Therefore, for those seeking CoQ10’s classic documented benefits, supplementing with 100-150 mg a day of ubiquinol would appear to be appropriate. Those who want to emulate the successful anti-senescence mouse study should consider a dose of 200-300 mg a day of ubiquinol. Since the anti-senescence study dose was based on food intake, those who restrict their calorie intake to around one kilo (2.2 pounds) a day would need only about 200 mg of ubiquinol, while those who consumed more calories would need to take 250-300 mg of ubiquinol. Reducing one’s food intake (without inducing malnutrition) is the single best-documented anti-aging therapy.85-91 In the case of ubiquinol requirements, those who eat sensibly would require less of this supplemental nutrient. SummaryThe lay public recognizes CoQ10 as a nutrient that protects heart health, yet provocative research indicates that CoQ10 may have a wide range of benefits that include preventing skin cancer and skin aging,33,58 guarding against prostate and breast cancers,29,36,64,92 supporting healthy blood sugar levels in diabetics,4,5 and averting endothelial dysfunction.93
Scientists also report additional novel uses of CoQ10, such as helping to slow the progression of Parkinson’s disease,47,94,95 preventing crippling migraine headaches,96,97 supporting immune health,98-100 guarding against periodontal disease,34,38 preserving healthy vision,28,101 and boosting male fertility.102 In what may be one of the most dramatic anti-aging discoveries to date, scientists have demonstrated that the ubiquinol form of CoQ10 provides anti-aging effects that are far superior to those associated with the conventional ubiquinone form used by millions of Americans each day. For the first time, ubiquinol is available as a stabilized dietary supplement that provides more activated coenzyme Q10 to the body—at a lower cost—than any other form of CoQ10.
| ||||||||||||||
| References | ||||||||||||||
| 1. Dhanasekaran M, Ren J. The emerging role of coenzyme Q-10 in aging, neurodegeneration, cardiovascular disease, cancer and diabetes mellitus. Curr Neurovasc Res. 2005 Dec;2(5):447-59. 2. Wang XL, Rainwater DL, Mahaney MC, Stocker R. Cosupplementation with vitamin E and coenzyme Q10 reduces circulating markers of inflammation in baboons. Am J Clin Nutr. 2004 Sep;80(3):649-55. 3. Rosenfeldt FL, Pepe S, Linnane A, et al. Coenzyme Q10 protects the aging heart against stress: studies in rats, human tissues, and patients. Ann NY Acad Sci. 2002 Apr;959:355-9. 4. Hodgson JM, Watts GF, Playford DA, Burke V, Croft KD. Coenzyme Q10 improves blood pressure and glycaemic control: a controlled trial in subjects with type 2 diabetes. Eur J Clin Nutr. 2002 Nov;56(11):1137-42. 5. Gaby AR. The role of coenzyme Q10 in clinical medicine: Part II. Cardiovascular disease, hypertension, diabetes mellitus and infertility. Altern Med Rev. 1996:1:168-75. 6. Singh RB, Niaz MA. Serum concentration of lipoprotein(a) decreases on treatment with hydrosoluble coenzyme Q10 in patients with coronary artery disease: discovery of a new role. Int J Cardiol. 1999 Jan;68(1):23-9. 7. Singh RB, Niaz MA, Rastogi SS, Shukla PK, Thakur AS. Effect of hydrosoluble coenzyme Q10 on blood pressures and insulin resistance in hypertensive patients with coronary artery disease. J Hum Hypertens. 1999 Mar;13(3):203-8. 8. Baggio E, Gandini R, Plancher AC, Passeri M, Carmosino G. Italian multicenter study on the safety and efficacy of coenzyme Q10 as adjunctive therapy in heart failure. CoQ10 Drug Surveillance Investigators. Mol Aspects Med. 1994;15 Suppls287-94. 9. Morisco C, Trimarco B, Condorelli M. Effect of coenzyme Q10 therapy in patients with congestive heart failure: a long-term multicenter randomized study. Clin Investig. 1993;71(8 Suppl):S134-6. 10. Greenberg S, Frishman WH. Co-enzyme Q10: a new drug for cardiovascular disease. J Clin Pharmacol. 1990 Jul;30(7):596-608. 11. Tran MT, Mitchell TM, Kennedy DT, Giles JT. Role of coenzyme Q10 in chronic heart failure, angina, and hypertension. Pharmacotherapy. 2001 Jul;21(7):797-806. 12. Munkholm H, Hansen HH, Rasmussen K. Coenzyme Q10 treatment in serious heart failure. Biofactors. 1999;9(2-4):285-9. 13. Hofman-Bang C, Rehnqvist N, Swedberg K, Wiklund I, Astrom H. Coenzyme Q10 as an adjunctive in the treatment of chronic congestive heart failure. The Q10 Study Group. J Card Fail. 1995 Mar;1(2):101-7. 14. Thomas SR, Leichtweis SB, Pettersson K, et al. Dietary cosupplementation with vitamin E and coenzyme Q(10) inhibits atherosclerosis in apolipoprotein E gene knockout mice. Arterioscler Thromb Vasc Biol. 2001 Apr;21(4):585-93. 15. Witting PK, Pettersson K, Letters J, Stocker R. Anti-atherogenic effect of coenzyme Q10 in apolipoprotein E gene knockout mice. Free Radic Biol Med. 2000 Aug;29(3-4):295-305. 16. Mortensen SA, Vadhanavikit S, Baandrup U, Folkers K. Long-term coenzyme Q10 therapy: a major advance in the management of resistant myocardial failure. Drugs Exp Clin Res. 1985;11(8):581-93. 17. Langsjoen PH, Vadhanavikit S, Folkers K. Effective treatment with coenzyme Q10 of patients with chronic myocardial disease. Drugs Exp Clin Res. 1985;11(8):577-9. 18. Furuta T, Kodama I, Kondo N, Toyama J, Yamada K. A protective effect of coenzyme Q10 on isolated rabbit ventricular muscle under hypoxic condition. J Cardiovasc Pharmacol. 1982 Nov;4(6):1062-7. 19. Yamagami T, Shibata N, Folkers K. Bioenergetics in clinical medicine. VIII. Adminstration of coenzyme Q10 to patients with essential hypertension. Res Commun Chem Pathol Pharmacol. 1976 Aug;14(4):721-7. 20. Somayajulu M, McCarthy S, Hung M, et al. Role of mitochondria in neuronal cell death induced by oxidative stress; neuroprotection by Coenzyme Q10. Neurobiol Dis. 2005 Apr;18(3):618-27. 21. Menke T, Gille G, Reber F, et al. Coenzyme Q10 reduces the toxicity of rotenone in neuronal cultures by preserving the mitochondrial membrane potential. Biofactors. 2003;18(1-4):65-72. 22. Matthews RT, Yang L, Browne S, Baik M, Beal MF. Coenzyme Q10 administration increases brain mitochondrial concentrations and exerts neuroprotective effects. Proc Natl Acad Sci USA. 1998 Jul 21;95(15):8892-7. 23. Beal MF, Matthews RT, Tieleman A, Shults CW. Coenzyme Q10 attenuates the 1-methyl-4-phenyl-1,2,3,tetrahydropyridine (MPTP) induced loss of striatal dopamine and dopaminergic axons in aged mice. Brain Res. 1998 Feb 2;783(1):109-14. 24. Ren Z, Ding W, Su Z, et al. Mechanisms of brain injury with deep hypothermic circulatory arrest and protective effects of coenzyme Q10. J Thorac Cardiovasc Surg. 1994 Jul;108(1):126-33. 25. Gazdikova K, Gvozdjakova A, Kucharska J et al. [Effect of coenzyme Q10 in patients with kidney diseases]. Cas Lek Cesk. 2001 May 24;140(10):307-310. 26. Okamoto H, Kawaguchi H, Togashi H, et al. Effect of coenzyme Q10 on structural alterations in the renal membrane of stroke-prone spontaneously hypertensive rats. Biochem Med Metab Biol. 1991 Apr;45(2):216-26. 27. Takenaka M, Tatsukawa Y, Dohi K, et al. Protective effects of alpha-tocopherol and coenzyme Q10 on warm ischemic damages of the rat kidney. Transplantation. 1981 Aug;32(2):137-41. 28. Feher J, Kovacs B, Kovacs I, et al. Improvement of visual functions and fundus alterations in early age-related macular degeneration treated with a combination of acetyl-L-carnitine, n-3 fatty acids, and coenzyme Q10. Ophthalmologica. 2005 May;219(3):154-66. 29. Quiles JL, Farquharson AJ, Ramirez-Tortosa MC, et al. Coenzyme Q differentially modulates phospholipid hydroperoxide glutathione peroxidase gene expression and free radicals production in malignant and non-malignant prostate cells. Biofactors. 2003;18(1-4):265-70. 30. Miquel J. Can antioxidant diet supplementation protect against age-related mitochondrial damage? Ann NY Acad Sci. 2002 Apr;959:508-16. 31. Linnane AW, Zhang C, Yarovaya N, et al. Human aging and global function of coenzyme Q10. Ann NY Acad Sci. 2002 Apr;959:396-411. 32. Linnane AW, Kopsidas G, Zhang C, et al. Cellular redox activity of coenzyme Q10: effect of CoQ10 supplementation on human skeletal muscle. Free Radic Res. 2002 Apr;36(4):445-53. 33. Hoppe U, Bergemann J, Diembeck W, et al. Coenzyme Q10, a cutaneous antioxidant and energizer. Biofactors. 1999;9(2-4):371-8. 34. Hanioka T, Tanaka M, Ojima M, Shizukuishi S, Folkers K. Effect of topical application of coenzyme Q10 on adult periodontitis. Mol Aspects Med. 1994;15 Suppls241-8. 35. Folkers K and Wolaniuk A. Research on coenzyme Q10 in clinical medicine and in immunomodulation. Drugs Exp Clin Res. 1985;11(8):539-45. 36. Suzuki H, Naitoh T, Kuniyoshi S, et al. Cardiac performance and coenzyme Q10 in thyroid disorders. Endocrinol Jpn. 1984 Dec;31(6):755-61. 37. Marubayashi S, Dohi K, Ezaki H, Hayashi K, Kawasaki T. Preservation of ischemic rat liver mitochondrial functions and liver viability with CoQ10. Surgery. 1982 Jun;91(6):631-7. 38. Wilkinson EG, Arnold RM, Folkers K, Hansen I, Kishi H. Bioenergetics in clinical medicine. II. Adjunctive treatment with coenzyme Q in periodontal therapy. Res Commun Chem Pathol Pharmacol. 1975 Sep;12(1):111-23. 39. Available at: http://www.patentstorm.us/patents/6184255-fulltext.html. Accessed October 23, 2006. 40. Weber C, Jakobsen TS, Mortensen SA, Paulsen G, Holmer G. Effect of dietary coenzyme Q10 as an antioxidant in human plasma. Mol Aspects Med. 1994;15 Suppls97-102. 41. Unpublished data, Kaneka Corp. 42. Kazunori H, Mitsuaki K, Hideyuki, K Hiroshi, K Kenji, F Mikio, K. Study on safety and bioavailability of ubiquinol (Kaneka QHtm). Regul Toxicol Pharmacol. 2006 Aug 17. 43. Langsjoen PH, Langsjoen AM. Overview of the use of CoQ10 in cardiovascular disease. Biofactors. 1999;9(2-4):273-84. 44. Ubiquinol has a higher bioavailability compared to ubiquinone. Unpublished data, Kaneka Corp. 45. Plasma levels of COQ10 for ubiquinol increased dose dependently. Unpublished data, Kaneka Corp. 46. Hosoe K, Kitano M, Kishida H, et al. Study on safety and bioavailability of ubiquinol (Kaneka QH(trade mark)) after single and 4-week multiple oral administration to healthy volunteers. Regul Toxicol Pharmacol. 2006 Aug 17. 47. Shults CW, Oakes D, Kieburtz K, et al. Effects of coenzyme Q10 in early Parkinson disease: evidence of slowing of the functional decline. Arch Neurol. 2002 Oct;59(10):1541-50. 48. Shults CW, Flint BM, Song D, Fontaine D. Pilot trial of high dosages of coenzyme Q10 in patients with Parkinson’s disease. Exp Neurol. 2004 Aug;188(2):491-4. 49. Kurowska EM, Dresser G, Deutsch L, Bassoo E, Freeman DJ. Relative bioavailability and antioxidant potential of two coenzyme q10 preparations. Ann Nutr Metab. 2003;47(1):16-21. 50. Shults CW, Haas RH, Beal MF. A possible role of coenzyme Q10 in the etiology and treatment of Parkinson’s disease. Biofactors. 1999;9(2-4):267-72. 51. Age difference of bioavailability. Unpublished data, Kaneka Corp. 52. CoQ10 reducing activity in rats. Unpublished data, Kaneka Corp. 53. Available at: http://cancerweb.ncl.ac.uk/cancernet/600916.html. Accessed October 19, 2006. 54. Ernster L, Forsmark-Andree P. Ubiquinol: an endogenous antioxidant in aerobic organisms. Clin Investig. 1993;71(8 Suppl):S60-5. 55. Passi S, De PO, Puddu P, Littarru GP. Lipophilic antioxidants in human sebum and aging. Free Radic Res. 2002 Apr;36(4):471-7. 56. Naini A, Lewis VJ, Hirano M, DiMauro S. Primary coenzyme Q10 deficiency and the brain. Biofactors. 2003;18(1-4):145-52. 57. Siemieniuk E and Skrzydlewska E. Coenzyme Q10: its biosynthesis and biological significance in animal organisms and in humans. Postepy Hig Med Dosw (Online). 2005;59:150-9. 58. Rusciani L, Proietti I, Rusciani A, et al. Low plasma coenzyme Q10 levels as an independent prognostic factor for melanoma progression. J Am Acad Dermatol. 2006 Feb;54(2):234-41. 59. Kontush A, Schippling S, Spranger T, Beisiegel U. Plasma ubiquinol-10 as a marker for disease: is the assay worthwhile? Biofactors. 1999;9(2-4):225-9. 60. Yamamoto Y, Yamashita S. Plasma ubiquinone to ubiquinol ratio in patients with hepatitis, cirrhosis, and hepatoma, and in patients treated with percutaneous transluminal coronary reperfusion. Biofactors. 1999;9(2-4):241-6. 61. Sohmiya M, Tanaka M, Suzuki Y, et al. An increase of oxidized coenzyme Q-10 occurs in the plasma of sporadic ALS patients. J Neurol Sci. 2005 Jan 15;228(1):49-53. 62. Folkers K, Osterborg A, Nylander M, Morita M, Mellstedt H. Activities of vitamin Q10 in animal models and a serious deficiency in patients with cancer. Biochem Biophys Res Commun. 1997 May 19;234(2):296-9. 63. Portakal O, Ozkaya O, Erden IM, et al. Coenzyme Q10 concentrations and antioxidant status in tissues of breast cancer patients. Clin Biochem. 2000 Jun;33(4):279-84. 64. Lockwood K, Moesgaard S, Yamamoto T, Folkers K. Progress on therapy of breast cancer with vitamin Q10 and the regression of metastases. Biochem Biophys Res Commun. 1995 Jul 6;212(1):172-7. 65. Lockwood K, Moesgaard S, Folkers K. Partial and complete regression of breast cancer in patients in relation to dosage of coenzyme Q10. Biochem Biophys Res Commun. 1994 Mar 30;199(3):1504-8. 66. Palan PR, Mikhail MS, Shaban DW, Romney SL. Plasma concentrations of coenzyme Q10 and tocopherols in cervical intraepithelial neoplasia and cervical cancer. Eur J Cancer Prev. 2003 Aug;12(4):321-6. 67. Jolliet P, Simon N, Barre J, et al. Plasma coenzyme Q10 concentrations in breast cancer: prognosis and therapeutic consequences. Int J Clin Pharmacol Ther. 1998 Sep;36(9):506-9. 68. Muller T, Buttner T, Gholipour AF, Kuhn W. Coenzyme Q10 supplementation provides mild symptomatic benefit in patients with Parkinson’s disease. Neurosci Lett. 2003 May 8;341(3):201-4. 69. Ferrante KL, Shefner J, Zhang H, et al. Tolerance of high-dose (3,000 mg/day) coenzyme Q10 in ALS. Neurology. 2005 Dec 13;65(11):1834-6. 70. Mariani C, Bresolin N, Farina E, et al. Muscle biopsy in Alzheimer’s disease: morphological and biochemical findings. Clin Neuropathol. 1991 Jul;10(4):171-6. 71. Koroshetz WJ, Jenkins BG, Rosen BR, Beal MF. Energy metabolism defects in Huntington’s disease and effects of coenzyme Q10. Ann Neurol. 1997 Feb;41(2):160-5. 72. Siciliano G, Mancuso M, Tedeschi D, et al. Coenzyme Q10, exercise lactate and CTG trinucleotide expansion in myotonic dystrophy. Brain Res Bull. 2001 Oct 1;56(3-4):405-10. 73. Folkers K, Simonsen R. Two successful double-blind trials with coenzyme Q10 (vitamin Q10) on muscular dystrophies and neurogenic atrophies. Biochim Biophys Acta. 1995 May 24;1271(1):281-6. 74. Yan J, Fujii K, Yao J, et al. Reduced coenzyme Q10 supplementation decelerates senescence in SAMP1 mice. Exp Gerontol. 2006 Feb;41(2):130-40. 75. Anti-fatigue effect in rats. Unpublished data, Kaneka Corp. 76. Anti-diabetic activity of Kaneka QH in rats. Unpublished data, Kaneka Corp. 77. Frei B, Kim MC, Ames BN. Ubiquinol-10 is an effective lipid-soluble antioxidant at physiological concentrations. Proc Natl Acad Sci USA. 1990 Jun;87(12):4879-83. 78. Bowry VW, Mohr D, Cleary J, Stocker R. Prevention of tocopherol-mediated peroxidation in ubiquinol-10-free human low density lipoprotein. J Biol Chem. 1995 Mar 17;270(11):5756-63. 79. Ingold KU, Bowry VW, Stocker R, Walling C. Autoxidation of lipids and antioxidation by alpha-tocopherol and ubiquinol in homogeneous solution and in aqueous dispersions of lipids: unrecognized consequences of lipid particle size as exemplified by oxidation of human low density lipoprotein. Proc Natl Acad Sci U S A. 1993 Jan 1;90(1):45-9. 80. Okamoto T, Matsuya T, Fukunaga Y, Kishi T, Yamagami T. Human serum ubiquinol-10 levels and relationship to serum lipids. Int J Vitam Nutr Res. 1989;59(3):288-92. 81. Mohr D, Bowry VW, Stocker R. Dietary supplementation with coenzyme Q10 results in increased levels of ubiquinol-10 within circulating lipoproteins and increased resistance of human low-density lipoprotein to the initiation of lipid peroxidation. Biochim Biophys Acta. 1992 Jun 26;1126(3):247-54. 82. Quinn PJ: Topography of coenzyme Q in membranes. In: Kagan VE, Quinn PJ, eds. Coenzyme Q: Molecular Mechanisms in Health and Disease. Boca Raton: CRC Press; 2001:29-42. 83. James AM, Cocheme HM, Smith RA, Murphy MP. Interactions of mitochondria-targeted and untargeted ubiquinones with the mitochondrial respiratory chain and reactive oxygen species. Implications for the use of exogenous ubiquinones as therapies and experimental tools. J Biol Chem. 2005 Jun 3;280(22):21295-312. 84. Szeto HH. Mitochondria-targeted peptide antioxidants: novel neuroprotective agents. AAPS J. 2006;8(3):E521-31. 85. Available at: http://www.nature.com/nature/journal/v414/n6862/abs/414412a0.html. Accessed October 12, 2006. 86. Ingram DK, Lane MA, Roth GS. Calorie restriction in monkeys. Life Extension. July, 1998:36-43. 87. Roth GS, Ingram DK, Lane MA. Calorie restriction in primates: will it work and how will we know? J Am Geriatr Soc. 1999 Jul;47(7):896-903. 88. Walford RL, Harris SB, Gunion MW. The calorically restricted low-fat nutrient-dense diet in Biosphere 2 significantly lowers blood glucose, total leukocyte count, cholesterol, and blood pressure in humans. Proc Natl Acad Sci USA. 1992 Dec 1;89(23):11533-7. 89. Lee CK, Klopp RG, Weindruch R, Prolla TA. Gene expression profile of aging and its retardation by caloric restriction. Science. 1999 Aug 27;285(5432):1390-3. 90. Weindruch R, Walford RL. Dietary restriction in mice beginning at 1 year of age: effect on life-span and spontaneous cancer incidence. Science. 1982 Mar 12;215(4538):1415-8. 91. Cao SX, Dhahbi JM, Mote PL, Spindler SR. Genomic profiling of short- and long-term caloric restriction effects in the liver of aging mice. Proc Natl Acad Sci USA. 2001 Sep 11;98(19):10630-5. 92. Larsson O. Effects of isoprenoids on growth of normal human mammary epithelial cells and breast cancer cells in vitro. Anticancer Res. 1994 Jan;14(1A):123-8. 93. Kuettner A, Pieper A, Koch J, Enzmann F, Schroeder S. Influence of coenzyme Q(10) and cerivastatin on the flow-mediated vasodilation of the brachial artery: results of the ENDOTACT study. Int J Cardiol. 2005 Feb 28;98(3):413-9. 94. Beal MF. Mitochondrial dysfunction and oxidative damage in Alzheimer’s and Parkinson’s diseases and coenzyme Q10 as a potential treatment. J Bioenerg Biomembr. 2004 Aug;36(4):381-6. 95. Baker SK, Tarnopolsky MA. Targeting cellular energy production in neurological disorders. Expert Opin Investig Drugs. 2003 Oct;12(10):1655-79. 96. Rozen TD, Oshinsky ML, Gebeline CA, et al. Open label trial of coenzyme Q10 as a migraine preventive. Cephalalgia. 2002 Mar;22(2):137-41. 97. Sandor PS, Di CL, Coppola G, et al. Efficacy of coenzyme Q10 in migraine prophylaxis: a randomized controlled trial. Neurology. 2005 Feb 22;64(4):713-5. 98. Gazdik F, Pijak MR, Borova A, Gazdikova K. Biological properties of coenzyme Q10 and its effects on immunity. Cas Lek Cesk. 2003;142(7):390-3. 99. Ye CQ, Folkers K, Tamagawa H, Pfeiffer C. A modified determination of coenzyme Q10 in human blood and CoQ10 blood levels in diverse patients with allergies. Biofactors. 1988 Dec;1(4):303-6. 100. Rosenfeldt FL, Mijch A, McCrystal G, et al. Skeletal myopathy associated with nucleoside reverse transcriptase inhibitor therapy: potential benefit of coenzyme Q10 therapy. Int J STD AIDS. 2005 Dec;16(12):827-9. 101. Blasi MA, Bovina C, Carella G, et al. Does coenzyme Q10 play a role in opposing oxidative stress in patients with age-related macular degeneration? Ophthalmologica. 2001 Jan;215(1):51-4. 102. Sheweita SA, Tilmisany AM, Al-Sawaf H. Mechanisms of male infertility: role of antioxidants. Curr Drug Metab. 2005 Oct;6(5):495-501. 103. Rosenfeldt FL, Pepe S, Ou R, et al. Coenzyme Q10 improves the tolerance of the senescent myocardium to aerobic and ischemic stress: studies in rats and in human atrial tissue. Biofactors. 199;9(2-4):291-9. 104. Kalen A, Appelkvist EL, Dallner G. Age-related changes in the lipid compositions of rat and human tissues. Lipids. 1989 Jul;24(7):579-84. 105. Hoppe U, Bergemann J, Diembeck W, et al. Coenzyme Q10, a cutaneous antioxidant and energizer. Biofactors. 1999;9(2-4):371-8. |





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Wellness
Specialists
1-800-226-2370 - This service is FREE
7:30 AM - 12 AM (ET) Mon-Fri | 9 AM - 12 AM (ET) Sat-Sun