Life Extension Magazine®
Vinpocetine is a novel dietary supplement derived from the lesser periwinkle plant Vinca minor. Better known in the US as an attractive garden border than a health aid, this plant has many useful derivatives that promote better health and quality of life. Since it was first synthesized in the late 1960s, vinpocetine has been used to maintain and improve brain health and cognition. It is widely used in Japan and many European countries to treat a number of cerebrovascular diseases. As a dietary supplement, vinpocetine offers potential neuroprotective effects as well. To understand how and why this phytonutrient works, it is important to understand a bit about normal and abnormal blood flow in the brain. Nourishing the BrainThe healthy adult brain receives fully one seventh of the heart’s output of blood every minute. This abundant blood flow is needed to provide the constant supply of oxygen, glucose, and other nutrients that this incredibly complex organ requires to function properly. Unlike most other body tissues such as muscle that can function reasonably well for several minutes without fresh oxygen, brain tissue is incapable of so-called “anaerobic metabolism.” Even a brief interruption in the delivery of oxygen to brain tissue results in almost immediate damage to brain cells. Fortunately, the brain is equipped with an excellent circulatory system of its own. Not unlike a modern jetliner with its multiple power backup systems, the brain has four major arteries to keep blood flowing. The two carotid arteries in the sides of the neck provide most of the blood flow to the front and top of the brain, while the vertebral arteries, which climb up through the spinal column, join together with parts of the carotids to form the Circle of Willis. This circle is critical, as it is the only area of the body where all four blood vessels join, allowing blood to be shunted to areas where it is needed, even if one of the major vessels becomes blocked. Like the body’s other blood vessels, the cerebral blood vessels suffer changes over time that can cause them to narrow. Atherosclerosis, or the accumulation of fat-laden, calcified plaque, is one of the most common causes of narrowing of the cerebral arteries. Chronic high blood pressure is another cause, as the steady pounding of high-pressure blood causes the muscular layer of the vessels to enlarge. With advancing age, blood vessels lose some of their elasticity as well, making it difficult for them to maintain and regulate blood flow. Finally, characteristics of blood itself can significantly affect its flow through brain blood vessels. Elevated levels of red blood cells, as occurs in dehydration and certain lung and kidney diseases, can make the blood thicker and more resistant to easy flow. Red blood cells and platelets also need to remain flexible to slip through tiny capillary openings and reach the tissue. Blood cell membranes lose flexibility under the influence of free radicals that oxidize some of their component lipids.
All of these factors can reduce blood flow to the brain. When an area suddenly stops getting adequate blood flow, the result is an ischemic stroke. Some tissue dies immediately, while other tissue, paradoxically, may be destroyed only when blood flow is restored, oxygen returns, and free radicals are generated that damage brain cell membranes. Many older adults have low levels of cerebral vascular disease, which leads to a condition called chronic cerebral vascular ischemia. In this condition, blood still gets to all areas of the brain, but some areas receive insufficient blood flow to support long-term function. Vascular dementia is the term for more advanced brain injury that results from inadequate flow to brain areas responsible for cognition. In a very recent study, total cerebral blood flow was found to be reduced even in apparently healthy elderly patients compared to younger adults, and it was more diminished still among elderly people with dementia.1 Alzheimer’s disease is probably not directly related to blood flow, but is thought to result from chronic exposure to toxic excitatory amino acids and free radical formation. Vinpocetine’s Effects on Brain HealthVinpocetine has effects on brain blood vessels, brain blood flow, and brain cells themselves. In this way, it can be of value in enhancing the delivery of oxygen and nutrients to the brain, as well as in possibly preventing the damage that occurs if nutrient delivery is impaired. Some research suggests that vinpocetine may also help to prevent the neurotoxic effects implicated in Alzheimer’s disease. Vinpocetine inhibits an enzyme called phosphodiesterase type 1 (PDE1) while reducing intracellular calcium levels, both of which normally cause smooth muscle in blood vessels to contract and narrow the diameter of the vessels. Inhibition of PDE1 and calcium thus allows brain blood vessels to relax and increases the amount of blood flowing through them.2-5 Many people are familiar with PDE5 inhibitors such as sildenafil or Viagra®, as well as calcium channel blockers such as diltiazem (Cardizem® and others). Those drugs also work to dilate blood vessels and maintain healthy blood flow in other parts of the body.
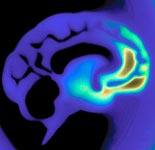
By inhibiting PDE1, as well as through its antioxidant properties,6-8 vinpocetine reduces the viscosity, or “stickiness,” of red blood cells and platelets.9-13 This allows blood to flow more easily through narrowed vessels, and may help to protect brain tissues in the event of transient loss of blood pressure, when the tissues might otherwise experience insufficient flow (the so-called “watershed stroke” caused by hypoperfusion). If blood flow to a region of the brain drops enough to cause cellular damage, there is still opportunity to protect nerve cells from both the immediate injury and the oxidant stress that follows when blood flow returns. Vinpocetine is a sodium channel blocker that may protect the cells from this “reperfusion” injury by preventing the accumulation of sodium in injured brain cells.7,14 This effect may also contribute to preserving brain cells’ ability to restructure themselves after an injury and to rapidly restore cognitive function.8 Since 1978, vinpocetine has been commonly used in many countries to treat cerebral vascular diseases.15,16 It is currently approved for use in tablet form in 47 countries.17 The evidence for its use is strongest in the treatment of chronic cerebral vascular ischemia, though growing evidence suggests that it may be beneficial in treating or preventing acute ischemic strokes and various forms of dementia. Chronic Cerebral Vascular IschemiaIn chronic vascular ischemia, it is important to increase blood flow to the affected areas to increase the delivery of both oxygen and glucose, the brain’s only source of energy.18 Using positron emission tomography (PET) scanning, Hungarian investigators demonstrated that administering vinpocetine led to an increase in glucose transport into the whole brain.2 Other researchers used PET scanning to demonstrate the effectiveness of either IV or oral tablet vinpocetine. They showed that vinpocetine increased brain glucose uptake and metabolism, especially in areas nearest the damaged tissue. Other studies using transcranial Doppler ultrasound and other techniques have also demonstrated increased regional blood flow and enhanced glucose supply to brain tissue in response to vinpocetine.7 Patients who took the oral tablet form of the supplement also showed an increase in blood flow in the injured regions.4 In a small double-blind, randomized, controlled trial, 14 days of vinpocetine given intravenously significantly increased cerebral blood flow in patients with chronic cerebral vascular ischemia.3 Of special importance, these investigators found that vinpocetine treatment helped to redistribute blood to the areas where it was needed most. These physiological effects seem to correlate with actual clinical improvements as well. In an early double-blind, placebo-controlled trial of vinpocetine in the treatment of chronic vascular ischemia, supplemented patients scored better on a battery of cognitive measures such as the Clinical Global Impression scale, the Sandoz Clinical Assessment-Geriatric scale, and the Mini-Mental Status Questionnaire. No serious side effects were found in this study.19 In a much larger randomized, placebo-controlled trial, patients who took 30 or 60 mg per day of oral vinpocetine for 16 weeks showed marked improvements on the Clinical Global Impression scale and on cognitive performance tests. Patients taking vinpocetine also demonstrated lower severity of illness in that study.20 A 2005 study examined vinpocetine’s effects on cognition and brain blood flow. Although the study was relatively small, with only 14 subjects taking vinpocetine and 12 taking placebo, its results suggest that blood vessel diameter was significantly larger in the vinpocetine group. The investigators also reported that vinpocetine users did not have any worsening on a test of short-term memory over the three months following the trial, whereas the placebo patients did.21 Acute Ischemic Stroke“Brain attack” is the term many physicians use to describe acute ischemic strokes, in which blood supply to a region of the brain is suddenly blocked. As with heart attacks, the immediate death of tissue in the absence of oxygen and nutrients is followed by worsening damage as flow returns and free radicals are generated. A review of studies of vinpocetine in acute ischemic stroke conducted before the mid-1990s found small sample sizes and inconclusive findings.15 More recently, however, in a group of acute ischemic stroke patients, a single IV dose of 20 mg of vinpocetine was shown to increase brain perfusion and oxygen extraction compared to placebo.22 Laboratory rats given vinpocetine 30 minutes after induced ischemic stroke had a 42% reduction in the size of the damaged area compared with untreated animals.23 The same authors report significant, dose-dependent protection from short- and long-term neurotoxicity caused by the excitatory amino acids glutamate and N-methyl-D-aspartic acid (NMDA). These data would seem to support a role for vinpocetine in acute treatment of stroke, and might be the basis for recommending its regular use in patients at high risk for acute stroke. A small, single-blind trial of IV vinpocetine within 72 hours of acute stroke onset showed that the risk of a poor outcome was reduced by 30-60% in the treated group. The treated group also had better scores on the National Institutes of Health Stroke Scale at a three-month follow-up evaluation. No significant adverse results were seen, and the authors concluded by recommending a full-scale, double-blind, placebo-controlled trial of vinpocetine treatment in acute ischemic stroke.24 Dementia and Alzheimer’sAn early analysis of seven small trials reported that patients with various forms of dementia who supplemented with vinpocetine became “more vivid” and saw improvements in their cognitive performance and daily activity.25 Because this was a report of multiple trials in differing categories of patients and with different outcome measures, it is difficult to draw any firm conclusions from it. A more recent and rigorous analysis of multiple trials of vinpocetine for cognitive impairment and dementia showed benefit associated with taking oral vinpocetine at doses of 30-60 mg per day.26 The number of patients treated for longer than six months was small, however, and because of variability in design and outcome measures in the three studies these authors reviewed, they concluded that there was inconclusive evidence for the use of vinpocetine in patients with dementia. These authors emphasized the need for larger clinical trials with clearly defined inclusion criteria and outcome measurements. Promising evidence from the laboratory suggests that vinpocetine protects brain tissue from the oxidative stress caused by the “Alzheimer’s protein” known as amyloid beta or Abeta.27 Because vinpocetine also blocks the NMDA receptors that are thought to be involved in the genesis of Alzheimer’s disease,28 vinpocetine supplements have a potential role in preventing Alzheimer’s.
Treating Hearing DisordersVinpocetine has long been used in Eastern Europe to treat various forms of hearing disorders. A 1986 review of eight independent studies of substances that enhance blood flow found that vinpocetine produced improvements in hearing as well as in “ringing” of the ears, or tinnitus, following trauma to the ear.29 A decade later, an open-label study of vinpocetine at a dose of 20 mg a day for 10 days following trauma to the ear showed that vinpocetine supported significant improvement in hearing and a decrease in tinnitus, with the best results seen in patients who took the supplement within one week of the injury.30 Vinpocetine may also have a role in preventing non-traumatic hearing loss. According to a 2003 study, pre-treatment with vinpocetine prevented hearing loss associated with the antibiotic gentamicin in 118 patients under treatment for tuberculosis.31 These effects make biological sense, as vinpocetine’s effect on tiny intracellular structures called microtubules helps brain cells restore function after injury,8 and microtubules are important in the hearing cells of the inner ear as well. Uses for Urinary IncontinenceThe human urinary bladder is composed entirely of smooth muscle, which is markedly affected by phosphodiesterase (PDE) function. Urinary incontinence is often the result of so-called “detrusor instability,” or bladder spasm. Drugs such as atropine and oxybutinin (Ditropan®) are often used in treating bladder spasm, but these anticholinergic medications have many unpleasant (and some dangerous) side effects, such as dry mouth, blurry vision, and heart palpitations. There has been increased interest recently in using vinpocetine to help regulate unstable detrusor muscle through its inhibition of PDE1. In laboratory studies, vinpocetine relaxed both animal and human bladder smooth muscle.32-34 Initial clinical data suggested that vinpocetine might be helpful in patients with urgency, urge incontinence, and possibly other kinds of incontinence.11 In a small trial among 19 patients, 58% reported improvements in clinical symptoms or bladder function tests.35 Vinpocetine has been recommended in several recent reviews of substances helpful in controlling female urinary incontinence.36,37
Supplement SynergyThe female sex hormone progesterone has recently been shown to increase the fluidity and flexibility of red blood cells, contributing to the ease with which they can flow through small capillaries.38 Progesterone is manufactured from the precursor pregnenolone. The combination of pregnenolone and vinpocetine may therefore be especially helpful in people with sluggish or deficient blood flow. SummaryVinpocetine is a supplement with a wide variety of biological effects. It causes relaxation of smooth muscle, dilation of blood vessels, and improved blood flow, all of which have beneficial health effects. It also provides protection for nerve cells deprived of oxygen and nutrients, and further protects those cells from oxidative stress when blood flow is restored. The supplement has had its greatest proven clinical benefit in patients with chronic cerebral vascular ischemia, and evidence is growing for its potential usefulness in acute stroke, various forms of dementia, and urinary incontinence. Even after more than two decades of extensive use in Europe and Asia, side effects and adverse events are rarely reported among people taking vinpocetine supplements. | |||||
| References | |||||
| 1. Spilt A, Weverling-Rijnsburger AW, Middelkoop HA, et al. Late-onset dementia: structural brain damage and total cerebral blood flow. Radiology. 2005 Sep;236(3):990-5. 2. Szakall S, Boros I, Balkay L, et al. Cerebral effects of a single dose of intravenous vinpocetine in chronic stroke patients: a PET study. J Neuroimaging. 1998 Oct;8(4):197-204. 3. Szilagyi G, Nagy Z, Balkay L, et al. Effects of vinpocetine on the redistribution of cerebral blood flow and glucose metabolism in chronic ischemic stroke patients: a PET study. J Neurol Sci. 2005 Mar 15;229-230:275-84. 4. Vas A, Gulyas B, Szabo Z, et al. Clinical and non-clinical investigations using positron emission tomography, near infrared spectroscopy and transcranial Doppler methods on the neuroprotective drug vinpocetine: a summary of evidences. J Neurol Sci. 2002 Nov 15;203-204:259-62. 5. Wu SN. Large-conductance Ca2+- activated K+ channels:physiological role and pharmacology. Curr Med Chem. 2003 Apr;10(8):649-61. 6. Stolc S. Indole derivatives as neuroprotectants. Life Sci. 1999;65(18-19):1943-50. 7. Bonoczk P, Gulyas B, dam-Vizi V, et al. Role of sodium channel inhibition in neuroprotection: effect of vinpocetine. Brain Res Bull. 2000 Oct;53(3):245-54. 8. Lendvai B, Zelles T, Rozsa B, Vizi ES. A vinca alkaloid enhances morphological dynamics of dendritic spines of neocortical layer 2/3 pyramidal cells. Brain Res Bull. 2003 Jan 15;59(4):257-60. 9. Chiu PJ, Tetzloff G, Ahn HS, Sybertz EJ. Comparative effects of vinpocetine and 8-Br-cyclic GMP on the contraction and 45Ca-fluxes in the rabbit aorta. Am J Hypertens. 1988 Jul;1(3 Pt 1):262-8. 10. Jones OM, Brading AF, McC Mortensen NJ. Phosphodiesterase inhibitors cause relaxation of the internal anal sphincter in vitro. Dis Colon Rectum. 2002 Apr;45(4):530-6. 11. Truss MC, Stief CG, Uckert S, et al. Phosphodiesterase 1 inhibition in the treatment of lower urinary tract dysfunction: from bench to bedside. World J Urol. 2001 Nov;19(5):344-50. 12. Mancina R, Filippi S, Marini M, et al. Expression and functional activity of phosphodiesterase type 5 in human and rabbit vas deferens. Mol Hum Reprod. 2005 Feb;11(2):107-15. 13. Szapary L, Horvath B, Alexy T, et al. Effect of vinpocetin on the hemorheologic parameters in patients with chronic cerebrovascular disease. Orv Hetil. 2003 May 18;144(20):973-8. 14. Molnar P, Erdo SL. Vinpocetine is as potent as phenytoin to block voltage-gated Na+ channels in rat cortical neurons. Eur J Pharmacol. 1995 Feb 6;273(3):303-6. 15. Bereczki D, Fekete I. A systematic review of vinpocetine therapy in acute ischaemic stroke. Eur J Clin Pharmacol. 1999 Jul;55(5):349-52. 16. Karpati E, Biro K, Kukorelli T. Investigation of vasoactive agents with indole skeletons at Richter Ltd. Acta Pharm Hung. 2002;72(1):25-36. 17. Anon. Vinpocetine. Monograph. Altern Med Rev. 2002 Jun;7(3):240-3. 18. Hadjiev D. Asymptomatic ischemic cerebrovascular disorders and neuroprotection with vinpocetine. Ideggyogy Sz. 2003 May 20;56(5-6):166-72. 19. Balestreri R, Fontana L, Astengo F. A double-blind placebo controlled evaluation of the safety and efficacy of vinpocetine in the treatment of patients with chronic vascular senile cerebral dysfunction. J Am Geriatr Soc. 1987 May;35(5):425-30. 20. Hindmarch I, Fuchs HH, Erzigkeit H. Efficacy and tolerance of vinpocetine in ambulant patients suffering from mild to moderate organic psychosyndromes. Int Clin Psychopharmacol. 1991;6(1):31-43. 21. Kemeny V, Molnar S, Andrejkovics M, Makai A, Csiba L. Acute and chronic effects of vinpocetine on cerebral hemodynamics and neuropsychological performance in multi-infarct patients. J Clin Pharmacol. 2005 Sep;45(9):1048-54. 22. Bonoczk P, Panczel G, Nagy Z. Vinpocetine increases cerebral blood flow and oxygenation in stroke patients: a near infrared spectroscopy and transcranial Doppler study. Eur J Ultrasound. 2002 Jun;15(1-2):85-91. 23. Dezsi L, Kis-Varga I, Nagy J, Komlodi Z, Karpati E. Neuroprotective effects of vinpocetine in vivo and in vitro. Apovincaminic acid derivatives as potential therapeutic tools in ischemic stroke. Acta Pharm Hung. 2002;72(2):84-91. 24. Feigin VL, Doronin BM, Popova TF, Gribatcheva EV, Tchervov DV. Vinpocetine treatment in acute ischaemic stroke: a pilot single-blind randomized clinical trial. Eur J Neurol. 2001 Jan;8(1):81-5. 25. Nagy Z, Vargha P, Kovacs L, Bonoczk P. Meta-analysis of Cavinton. Praxis. 1988 September 15;7(9):63-8. 26. Szatmari SZ, Whitehouse PJ. Vinpocetine for cognitive impairment and dementia. Cochrane Database Syst Rev. 2003;(1):CD003119. 27. Pereira C, Agostinho P, Oliveira CR. Vinpocetine attenuates the metabolic dysfunction induced by amyloid beta-peptides in PC12 cells. Free Radic Res. 2000 Nov;33(5):497-506. 28. Kiss B, Cai NS, Erdo SL. Vinpocetine preferentially antagonizes quisqualate/AMPA receptor responses: evidence from release and ligand binding studies. Eur J Pharmacol. 1991 Dec 10;209(1-2):109-12. 29. Pilgramm M, Schumann K. Need for rheologically active, vasoactive and metabolically active substances in the initial treatment of acute acoustic trauma. HNO. 1986 Oct;34(10):424-8. 30. Konopka W, Zalewski P, Olszewski J, Olszewska-Ziaber A, Pietkiewicz P. Treatment results of acoustic trauma. Otolaryngol Pol. 1997;51 Suppl 25:281-4. 31. Maliavina US, Ovchinnikov I, Fasenko VP, et al. Cavinton prevention of neurosensory hypoacousis in patients with different forms of tuberculosis. Vestn Otorinolaringol. 2003;(3):35-40. 32. Qiu Y, Kraft P, Craig EC, Liu X, Haynes-Johnson D. Cyclic nucleotide phosphodiesterases in rabbit detrusor smooth muscle. Urology. 2002 Jan;59(1):145-9. 33. Qiu Y, Kraft P, Craig EC, Liu X, Haynes-Johnson D. Identification and functional study of phosphodiesterases in rat urinary bladder. Urol Res. 2001 Dec;29(6):388-92. 34. Uckert S, Stief CG, Odenthal KP, et al. Comparison of the effects of various spasmolytic drugs on isolated human and porcine detrusor smooth muscle. Arzneimittelforschung. 1998 Aug;48(8):836-9. 35. Truss MC, Stief CG, Uckert S, et al. Initial clinical experience with the selective phosphodiesterase-I isoenzyme inhibitor vinpocetine in the treatment of urge incontinence and low compliance bladder. World J Urol. 2000 Dec;18(6):439-43. 36. Hampel C, Gillitzer R, Pahernik S, Melchior SW, Thuroff JW. Drug therapy of female urinary incontinence. Urologe A. 2005 Mar;44(3):244-55. 37. Alberti C. Bladder and cavernous contractility and relaxation among intracellular messengers, changes in sarcoplasmatic free calcium and phosphodiesterase activity. Arch Ital Urol Androl. 2000 Jun;72(2):75-82. 38. Tsuda K, Kinoshita Y, Nishio I. Synergistic role of progesterone and nitric oxide in the regulation of membrane fluidity of erythrocytes in humans: an electron paramagnetic resonance investigation. Am J Hypertens. 2002 Aug;15(8):702-8. |




Wellness
Specialists
1-800-226-2370 - This service is FREE
7:30 AM - 12 AM (ET) Mon-Fri | 9 AM - 12 AM (ET) Sat-Sun