Life Extension Magazine®
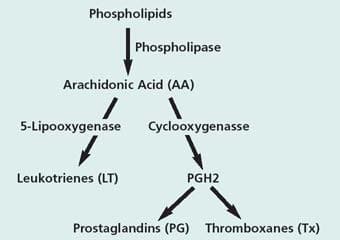
Pharmaceutical companies proclaimed a new era in arthritis management with the advent of the COX-2 inhibitors such as Celebrex® and Vioxx®. Unfortunately, these drugs work against themselves by upsetting the system of checks and balances through which the body regulates inflammation. A brief review of arthritis and the biochemical pathways leading to inflammation will help us understand the fly in this ointment—and what we can do about it. Aging and arthritis seem to go hand in hand. Arthritis is not a single disease, but rather a host of conditions that adversely affect the joints. Osteoarthritis is the most common form, affecting approximately 70% to 80% of the population over age 50. The onset is marked by morning stiffness, crackling joints and perhaps some pain. As it gets worse, it causes discomfort, pain and disability in varying degrees for millions of people. New research is beginning to shed light on how osteoarthritis develops at the cellular and molecular levels. Evidence is accumulating that the culprits are proinflammatory cytokines, together with the enzymes that generate inflammatory mediators and break down the collagen matrix. Cytokines are proteins that carry messages between cells and regulate immunity and inflammation. Two cytokines, tumor necrosis factor alpha (TNF-alpha) and interleukin one beta (IL-1 beta), play an essential role in the cartilage destruction and inflammation process.[1] They have been found in elevated levels in the synovial membrane, the synovial fluid and the cartilage of osteoarthritis patients. In animal models, it was shown that inhibition of TNF-alpha results in decreased inflammation, while inhibition of IL-1 beta effectively prevents cartilage destruction.[2] TNF-alpha has proven to be even more important in rheumatoid arthritis, where it is a key factor in promoting inflammation and damage to cartilage and bone.[3,4] Arthritis is almost certainly more common today than it was among our prehistoric ancestors. Its prevalence is most likely due to two facts of modern life: we live longer today and more of us are obese than ever before. However, effective treatments are now available that combine up-to-the-minute pharmacological advances with ancient herbal remedies. These remedies not only provide symptomatic pain relief, but also reverse the degenerative process itself. Inflammatory Pathways The rub is that inhibition of COX-2 is thought to lead to an imbalance between two key inflammatory mediators, raising levels of thromboxane A2 relative to prostaglandin E2. This in turn increases production of the above mentioned proinflammatory signaling molecules, the cytokines TNF- alpha (tumor necrosis factor alpha) and IL-1b (interleukin-1 beta).[5] In addition, there is evidence that elevated thromboxane A2 raises levels of an important inflammatory mediator in the LOX (lipoxygenase) pathway, leukotriene B4.[6] Thus COX-2 inhibition may help perpetuate the underlying degenerative process while relieving its superficial symptoms. As the scientists who made this discovery put it, “the short-term effects of (COX-2 inhibitors) on the pain and swelling of inflammation and arthritis may be achieved at the cost of an increased propensity to long-term tissue damage with which these cytokines have been associated.”[5] Another prominent researcher writes, “Tumor necrosis factor (TNF) and interleukin-1 (IL-1) are considered to be master cytokines in chronic, destructive arthritis.”[7] Their destructive roles overlap, however. In rheumatoid arthritis, TNF-alpha figures more prominently in triggering inflammation both locally and systemically, while IL-1 beta is more involved in destruction of cartilage and bone, and in impeding the repair of cartilage.[8] This research points up the importance of inhibiting TNF-alpha, IL-1 beta, and the LOX pathway when using a COX-2 inhibitor. Nettle Leaf Extract Nettle “may inhibit the inflammatory cascade in autoimmune diseases and rheumatoid arthritis,” concluded a team of researchers.[10] It is interesting to note that the prescription drug Enbrel®, approved for the treatment of rheumatoid arthritis, acts by suppressing TNF-alpha. One of the ways nettle leaf extract blocks proinflammatory signaling is by inhibiting the genetic transcription factor that activates TNF-alpha and IL-1 beta in synovial tissue.[11] This proinflammatory transcription factor, known as nuclear factor kappa beta (NF-kb), is elevated in chronic inflammatory diseases and is essential to activation of TNF-alpha. Nettle is thought to work by preventing degradation of the natural inhibitor of NF-kb in the body. TNF-alpha also activates NF-kb in synovial cells, leading to the suggestion that a cycle of cross-activation between TNF-alpha and NF-kb may sustain and amplify the disease process in rheumatoid arthritis.[12] A recent laboratory experiment revealed one of the mechanisms by which nettle leaf extract protects joints. Inflammatory joint diseases are characterized by breakdown of the extracellular matrix (ECM), which surrounds and supports cells. In arthritis, TNF-alpha and especially IL-1 beta stimulate enzymes known as matrix metalloproteinases (MMP’s) that break down the extracellular matrix. The experiment measured MMP levels of chondrocytes (joint cells) exposed to IL-1 beta. Nettle leaf extract was found to significantly inhibit all the matrix metalloproteinases tested (MMP-1, -3 and -9).[13] Another study conducted on 40 patients suffering from acute arthritis compared the effects of 200 mg of the nonsteroidal anti-inflammatory drug (NSAID) diclofenac with 50 mg of the NSAID in combination with 50 g of stewed nettle leaf per day.[14] Total joint scores improved significantly in both groups by approximately 70%. The nettle leaf extract clearly enhanced the anti-inflammatory effect of the NSAID. The addition of nettle extract made possible a 75% dose reduction of the NSAID, while still retaining the same anti-inflammatory effect with reduced side effects. Nettle leaf extract thus makes the ideal complement to COX-2 inhibitors, by virtue of its ability to counteract their negative effects. The herbal COX-2 inhibitor Nexrutine® is derived from the bark of the phellodendron tree, which folk healers use to treat arthritis and other ailments. Prescription COX-2 inhibitors intervene in the inflammation cascade by blocking the action of the COX-2 enzyme. But Nexrutine® inhibits the gene expression of COX-2, preventing its manufacture in the first place. This difference in mechanism of action may account for the rapidity of Nexrutine®’s inflammation-quenching action. According to reports from subjects who used Nexrutine® for two weeks, 79% agreed that Nexrutine® helped relieve or avoid the general aches and pains associated with overexertion and physical activity. No side effects were reported at recommended dosages.[15] |
Dual Inflammatory Pathway Blockade The problem with these drug candidates is that they block both forms of COX (COX-1 and COX-2) in addition to 5-LOX. Research has shown that indiscriminate COX inhibitors create a persistent “rebound effect” on proinflammatory signaling. Even two weeks after discontinuation of daily aspirin or ibuprofen, cytokine-stimulated production of TNF-alpha and IL-1 beta was increased from 270% to 538%.[17] Thus indiscriminate inhibitors of COX cause the same end result discussed above—potentiation of the two pivotal cytokines responsible for cartilage destruction and the inflammatory cascade in arthritis.
The balanced approach we have discussed—selective inhibition of COX-2 combined with inhibition of TNF-alpha and IL-1 beta—is, however, still incomplete. It is necessary to block the second inflammatory pathway, 5-lipoxygenase (5-LOX), which produces proinflammatory leukotrienes. Fortunately, an herbal inhibitor of 5-LOX has been discovered. 5-Loxin™ is derived from Boswellia serrata, a tree native to India whose aromatic gum resins have been used by practitioners of the Ayurvedic system of medicine to treat arthritis for centuries. Laboratory analysis of the gummy resin from Boswellia shows that one component, ß-boswellic acid, acts as a specific inhibitor of 5-LOX.[18] Having isolated and concentrated the most active of the Boswellic acids, it is now possible to derive the benefits of 5-LOX inhibition without consuming large amounts of ordinary Boswellia serrata extracts. A drug candidate under development by Shionogi, a Japanese pharmaceutical company, illustrates the potential of dual inflammatory pathway blockade. S-2474 is a dual inhibitor of COX-2 and 5-LOX. Not surprisingly, S-2474 significantly inhibited experimentally induced edema and arthritis while suppressing inflammatory mediators, all without ulcerogenic effects.[19] Demonstrating the pervasiveness of dual inflammatory pathways in degenerative processes in the body, S-2474 also protected brain cells from amyloid beta induced neuronal death. Amyloid beta, which gives rise to the “senile plaques” characteristic of Alzheimer’s disease, generates the proinflammatory prostaglandin D2 that was inhibited by S-2474.[20] A common herb, ginger root, contains gingerols that also inhibit both the cyclooxygenase and lipoxygenase pathways, and the production of prostaglandins, thromboxane and leukotrienes.[21-23] When COX-2 and 5-LOX inhibitors are used in tandem, inflammatory leukotrienes and prostaglandins are suppressed equally and balance is achieved safely. Rebuilding Joints Glucosamine is a naturally occurring substance in the body, synthesized in the chondrocytes. In osteoarthritis, this synthesis is defective and insufficient, and supplementation with glucosamine has proven to be useful. The body uses supplemental glucosamine to synthesize the proteoglycans and the water-binding glycosaminoglycans (GAGs) in the cartilage matrix. In addition to providing raw material, the presence of glucosamine seems to stimulate the chondrocytes in their production of these substances. Glucosamine also inhibits certain enzymes that destroy the cartilage, e.g., collagenase and phospholipase. By blocking pathogenic mechanisms that lead to articular degeneration, glucosamine delays the progression of the disease and relieves symptoms even for weeks after termination of the treatment.[24] Chondroitin sulfate is a major component of cartilage. It is a very large molecule, composed of repeated units of glucosamine sulfate. Like glucosamine, chondroitin sulfate has the ability to prevent enzymes from dissolving cartilage. Glucosamine alone or in combination with chondroitin sulfate is becoming recognized as the treatment of choice for osteoarthritis in the United States. Its ability to actually repair and improve joint function in addition to providing pain relief gives it a significant advantage over conventional treatment. Extensive studies have proven the ability of these natural tissue components to stimulate new tissue growth and suppress the enzymes that otherwise break down cartilage. A new study analyzed glucosamine and chondroitin clinical trials for knee osteoarthritis from 1980 through early 2002 through a sophisticated statistical technique known as “meta-analysis.” Glucosamine studies demonstrated a highly significant efficacy on all outcomes, including the WOMAC scale (Western Ontario MacMaster Univ. Osteoporosis Index) and joint space narrowing. Chondroitin was found effective on mobility, visual analog scale pain, the Lequesne Index of severity for osteoarthritis and responding status.[25] In order to maintain optimal joint health well into your later years, it’s important to maintain healthy weight and to exercise regularly. Overtaxed joints and weak muscles are a dangerous combination. Chondroitin and glucosamine sulfates can safely halt and reverse structural damage to joints, and promote the building of healthy new cartilage. Just as arthritis is not one condition, no single treatment is likely to yield satisfactory results. A systemic approach targeting proinflammatory cytokines, the dual inflammatory pathways and cartilage destruction should more effectively address the multifaceted nature of the host of conditions that are known as arthritis. | |||||
References | |||||
| 1. Feldmann M, et al. Role of cytokines in rheumatoid arthritis. Annu Rev Immunol. 1996; 14: 397-440. |
Wellness
Specialists
1-800-226-2370 - This service is FREE
7:30 AM - 12 AM (ET) Mon-Fri | 9 AM - 12 AM (ET) Sat-Sun