Life Extension Magazine®

Inflammation and Heart Disease
A growing consensus amongst scientists is that common disorders such as atherosclerosis, colon cancer and Alzheimer’s disease are all caused in part by a chronic inflammatory syndrome.
The New England Journal of Medicine recently published three articles showing that the presence of blood indicators of inflammation are strong predictive factors for determining who will develop coronary artery disease and suffer cardiac-related death.1-3
The good news is that many of the supplements used by Life Extension Foundation members appear to suppress these dangerous inflammatory components of blood.
One of the inflammatory markers the New England Journal of Medicine identified is a protein called fibrinogen. High fibrinogen levels can induce a heart attack via several mechanisms, including increased platelet aggregation, hyper-coagulation and excessive blood thickening. The New England Journal of Medicine studies showed that those with high levels of fibrinogen were more than twice as likely to die of a heart attack.
Another inflammatory marker reported on was C-reactive protein. This marker indicates an increased risk for destabilized atherosclerotic plaque and abnormal arterial clotting. When arterial plaque becomes destabilized, it can burst open and block the flow of blood through a coronary artery, resulting in an acute heart attack. One of The New England Journal of Medicine studies showed that people with high levels of C-reactive protein were almost three times as likely to die from a heart attack.
Why cardiologists are so slow to react
It was back in 1996 that The Life Extension Foundation published an article showing that high levels of fibrinogen represented a significant risk factor for heart attack and ischemic stroke.4 The Foundation’s based its report on studies dating back to the 1980’s showing that people with elevated fibrinogen levels were more likely to die from a cardiovascular-related disease.
Despite numerous studies linking elevated fibrinogen to increased heart attack risk, few doctors bother to check their patients blood levels of fibrinogen or other correctable risk factors such as homocysteine and C-reactive protein.
When The Life Extension Foundation challenges physicians to incorporate these published findings into their clinical practice, a common response from doctors who appreciate the importance of these tests is that managed care (HMOs and PPOs) refuse to pay for them. Other doctors demand a higher standard of proof before they test their patient’s blood for what they consider to be “newly identified” cardiac risk factors.
The sad fact is that the majority of practicing physicians are not even aware of these documented methods of measuring cardiovascular risk factors such as C-reactive protein, fibrinogen and homocysteine in the blood.
As a result of physician ignorance or insurance company stinginess, many Americans suffer progressive debilitating congestive heart failure or cerebral circulatory impairment when the underlying causes could be corrected if the physician ordered and properly interpreted these blood tests.
Correcting inflammatory risk factors

{kind=link}
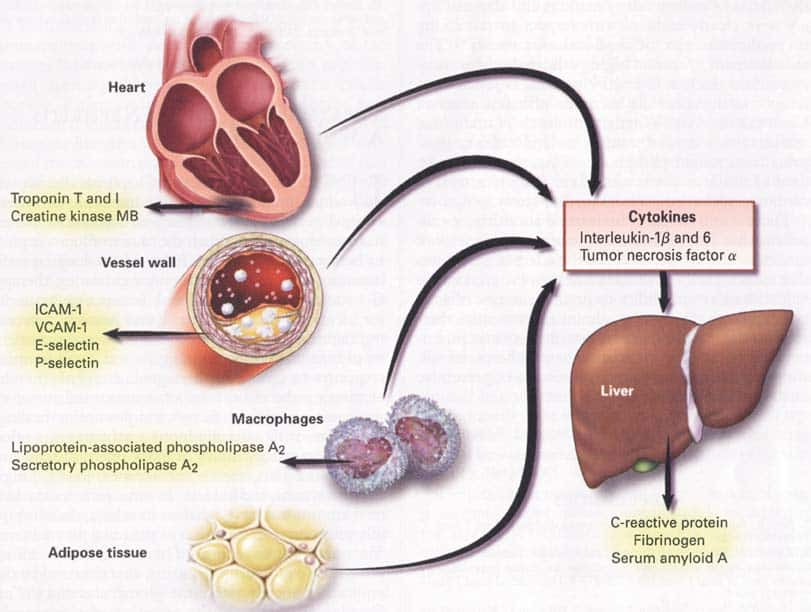
Sources of Inflammatory Markers and
Cytokines. New England Journal of
Medicine, October 19, 2000.
Reprinted with permission.
Cardiovascular risk factors such as fibrinogen and C-reactive protein are produced in the liver by pro-inflammatory cytokines called interleukin-1B, interleukin-6 and tumor necrosis factor alpha.4 For many years, Life Extension members have taken supplements such as DHEA to suppress excess production of some of these dangerous cytokines.
One recent study showed that interleukin-6 by itself increased the risk of heart attack, even after adjustment for the elevation in C-reactive protein induced by interleukin-6.3 Both vitamin K and DHEA suppress interleukin-6, which helps explain why these supplements have been shown to protect against such a wide range of age-related diseases.6-8
As far as suppressing the dangerous tumor necrosis factor alpha and interleukin-1B cytokines, nettle leaf extract appears to be the most effective dietary supplement.9-10 Nettle leaf extract is found in two popular formulas used by Foundation members.
Protect against fibrinogen-induced heart attack
Agents that inhibit platelet aggregation reduce the risk that fibrinogen will cause an abnormal arterial blood clot. Platelet aggregation inhibitors include aspirin, green tea, ginkgo, garlic and vitamin E.11-21 For optimal protection against the formation of arterial blood clots, it makes sense to utilize therapies that directly lower elevated fibrinogen levels.
High serum vitamin A and beta-carotene levels have been associated with reduced fibrinogen levels in humans. Animals fed a vitamin A deficient diet have an impaired ability to break down fibrinogen. When animals are injected with vitamin A, they produce tissue plasminogen activator (tPA), which breaks down fibrinogen.22-29
High doses of fish or olive oil have been shown to lower fibrinogen in humans with elevated fibrinogen levels.30-31 Excessive homocysteine blocks the natural breakdown of fibrinogen by inhibiting the production of tissue plasminogen activator (tPA).32 Folic acid, TMG, vitamin B12 and vitamin B6 reduce elevated homocysteine levels.
Vitamin C, in pharmacological doses, has been shown to break down excess fibrinogen. In one study, heart disease patients were given either 1000 mg or 2000 mg a day of vitamin C to measure the fibrinogen breakdown effect.
At 1000 mg a day, there was no detectable change in fibrinolytic activity or cholesterol. At 2000 mg a day of vitamin C, there was a 27% decrease in the platelet aggregation index, a 12% reduction in total cholesterol and a 45% increase in fibrinolysis (fibrinogen breakdown) activity.5
An additional marker of heart attack risk
Troponin T is a blood marker of heart muscle damage. A recent study showed this marker is the most powerful long-term predictor of cardiac death in those suffering from underlying heart disease. Compared to patients with the lowest levels of troponin T, those with the highest troponin T blood levels were almost 13 times more likely to die over a 37-month period.2 Why is troponin T such a powerful predictor? It turns out that even those with a minor elevation of troponin T have a larger number of tiny coronary artery blood clots, complex atherosclerotic coronary artery lesions and impaired coronary artery blood flow. Those with elevated troponin T levels, therefore, are the heart attack patients most likely to benefit from antiplatelet and antithrombotic therapies.
The type of “troponin” blood test preferred by most clinical laboratories is called Troponin I.” The Troponin I test is considered a more stable and predictable method of measurement in those with existing cardiovascular disease than troponin T.
Taking charge of your own health
As The Life Extension Foundation forges ahead in identifying better methods of protecting against degenerative disease, it has become increasingly apparent that members will have to take a more active role in protecting their health. That means those who are concerned about optimal health are going to have to stand up to their doctors and demand that certain blood and other diagnostic tests be performed, whether their physician agrees with them or not! It is high time that humans stop sacrificing their lives because of the inability of doctors and insurance companies to recognize diagnostic approaches that are substantiated in respected medical journals.
For members who are unable to secure physician-insurance company cooperation, we are pleased to announce that the cost of blood testing has come down considerably. Since 1996, Life Extension members throughout the United States have been able to order their own tests directly from the Foundation. This mail-order blood testing has enabled members to identify underlying risk factors that if corrected in time, could prevent a lethal disease from developing or worsening.
A medical center that will practice scientific medicine
While blood testing is important, so is comprehensive medical care that evaluates every diagnostic test result to bring each individual to an optimal state of health. The failure of managed care to provide holistic healthcare, based on what is already published in mainstream medical journals, is one of the purposes for establishing The Life Extension Medical Center, which is scheduled to open in Ft. Lauderdale, Florida in early 2001.
At The Life Extension Medical Center, the results of studies that are published in peer-reviewed medical and scientific journals will be used to develop novel approaches to prevent and treat the diseases of aging. It is our contention that managed care, physician apathy and FDA over-regulation is a lethal combination that is causing over one million Americans to needlessly die every single year. We believe the innovative approaches that will be practiced at The Life Extension Medical Center will save many lives.
In the meantime, those with chronic degenerative disease should take a pro-active role in their health care. If your physician does not appear to care about keeping you in an optimal state of health, find another doctor! Don’t become a victim of the current broken-down healthcare system that fails to incorporate scientific findings into the clinical practice of medicine.
In this issue of Life Extension, we present detailed findings about a highly promising anti-aging supplement. In preparing these articles, we reviewed a huge number of published studies in order to validate this novel scientific approach to help prevent the multiple pathological disorders involved in aging.
For longer life,
![]()
William Faloon
Life Extension Foundation
Testing your blood to avoid cardiovascular disease
Don't let complacent doctors put you at risk for heart disease and stroke. The following chart shows the most common blood tests that can help reveal underlying cardiovascular disease risk factors.
As can be seen on the chart below, blood test results that conventional doctors accept as being "normal" can be lethal to you. In other words, what the "Standard Reference Range" allows is not always a practical indicator for where your "optimal" level should be.
In many cases, a "Standard Reference Range" reflects what is expected to be seen in the average population. Since cardiovascular disease remains the number one killer of Americans, you don't ever want to be part of the "average" range when it comes to cardiovascular disease risk factors.
By keeping your blood levels in the "Optimal Range," rather than the average "Standard Reference Range," you take advantage of the increasing volume of evidence showing that most heart attacks and strokes are preventable.
As you can see, the "Standard Reference Range" often dangerously differs from what the published research indicates is protective against cardiovascular disease.
Blood Test |
What The "Standard Reference Range" Allows |
The "Optimal" Level Where YOU Want To Be |
| Fibrinogen | Up to 460 mg/dL |
Between 295-369 mg/dL |
| C-reactive protein | Up to 4.9 mg/L |
Under 2 mg/L Some studies indicate C-reactive protein levels should be below 1.3 mg/L(33,34) |
| Homocysteine | Up to 15 micro mol/L |
Under 7 micro mol/L |
| Glucose | Up to 109 mg/dL |
Under 100 mg/dL |
| Iron | Up to 180 mg/dL |
Under 100 mcg/dL |
| Cholesterol | Up to 199 mg/dL |
Between 180-220 mg/dL |
| LDL cholesterol | Up to 129 mg/dL |
Under 100 mg/dL |
| HDL cholesterol | No lower than 35 mg/dL |
Over 50 mg/dL |
| Triglycerides | Up to 199 mg/dL |
Under 100 mg/dL |
| DHEA | Males: No lower than 80 mcg/dL |
Between 400-560 mcg/dL |
Females: No lower than 35 mcg/dL |
Between 350-430 mcg/dL |
*There are numerous published studies indicating that cholesterol levels should ideally be under 200. The Life Extension Foundation believes it is more important to concentrate on suppressing dangerous LDL cholesterol and increasing beneficial HDL levels. If other risk factors such as homocysteine, fibrinogen, C-reactive protein, etc. are individually adjusted to reflect "optimal" ranges, then a slightly higher total cholesterol of up to 220 might be acceptable. Please note that cholesterol levels below 180 present increased risk of hemorrhagic stroke and other diseases, so it is important that people maintain a minimal amount of cholesterol, i.e. 180 milligrams per deciliter of blood. It is important to note that in the past, cholesterol levels well above 200 were considered within the "normal" reference range.
Note: For those with existing cardiovascular disease, the Troponin I blood test is highly recommended. Optimal levels are under 0.4 ng/mL, intermediate levels are between 0.5 and 1.9 ng/ml and dangerously high levels are considered over 2.0 ng/ml. Based on an extrapolation of the most recent New England Journal of Medicine study35, cardiac patients with troponin I levels over 0.4 ng/mL should ask their cardiologists to consider antiplatelet or antithrombotic therapy. In The New England Journal of Medicine study, those with troponin T levels in the intermediate range were seven times more likely to die over a 37-month period, while cardiac patients with troponin T levels above the intermediate range were almost 13 times as likely to die over a 37-month period.
References
- Packard CJ, et al. Lipoprotein-associated phospholipase A2 as an independent predictor of coronary heart disease. West of Scotland Coronary Prevention Study Group. N Engl J Med 2000 Oct 19;343(16):1148-55.
- Lindahl B, et al. Markers of myocardial damage and inflammation in relation to long-term mortality in unstable coronary artery disease. FRISC Study Group. Fragmin during Instability in Coronary Artery Disease. N Engl J Med 2000 Oct 19;343(16):1139-47.
- Rader DJ. Inflammatory markers of coronary risk. N Engl J Med 2000 Oct 19;343(16):1179-82.
- Ridker PM, et al. Plasma concentration of interleukin-6 and the risk of future myocardial infarction among apparently healthy men. Circulation 2000 Apr 18;101(15):1767-72.
- Bordia AK. The effect of vitamin C on blood lipids, fibrinolytic activity and platelet adhesiveness in patients with coronary artery disease. Atherosclerosis 1980 Feb;35(2):181-7.
- Kipper-Galperin M, et al. Dehydroepiandrosterone selectively inhibits production of tumor necrosis factor alpha and interleukin-6 [correction of interlukin-6] in astrocytes. Int J Dev Neurosci 1999 Dec;17(8):765-75.
- Haden ST, et al. Effects of age on serum dehydroepiandrosterone sulfate, IGF-I, and IL-6 levels in women. Calcif Tissue Int 2000 Jun;66(6):414-8.
- Reddi K, et al. Interleukin 6 production by lipopolysaccharide-stimulated human fibroblasts is potently inhibited by naphthoquinone (vitamin K) compounds. Cytokine 1995 Apr;7(3):287-90.
- eucher T, et al. [Cytokine secretion in whole blood of healthy subjects following oral administration of Urtica dioica L. plant extract]. Arzneimittelforschung 1996 Sep;46(9):906-10.
- Obertreis B, et al. Ex-vivo in-vitro inhibition of lipopolysaccharide stimulated tumor necrosis factor-alpha and interleukin-1 beta secretion in human whole blood by extractum urticae dioicae foliorum. Arzneimittelforschung 1996 Apr;46(4):389-94. Published erratum appears in Arzneimittelforschung 1996 Sep;46(9):936.
- Bossavy JP, et al. A double-blind randomized comparison of combined aspirin and ticlopidine therapy versus aspirin or ticlopidine alone on experimental arterial thrombogenesis in humans. Blood (UNITED STATES) Sep 1 1998 , 92 (5) p1518-25.
- Willoughby S; et al. The use of aspirin in polycythaemia vera and primary thrombocythaemia. Blood Rev (SCOTLAND) Mar 1998 , 12 (1) p12-22.
- Lopez-Farre A, et al.Thrombosis and coronary disease: neutrophils, nitric oxide and aspirin] Rev Esp Cardiol (SPAIN) Mar 1998 , 51 (3) p171-7.
- Kim YH, et al. Prophylaxis for deep vein thrombosis with aspirin or low molecular weight dextran in Korean patients undergoing total hip replacement. A randomized controlled trial. Int Orthop (GERMANY) 1998, 22 (1) p6-10.
- Shiflett S.C. Overview of complementary therapies in physical medicine and rehabilitation. Physical Medicine and Rehabilitation Clinics of North America 1999 10:3 (521-529).
- Stocker A, et al. Specific cellular responses to alpha-tocopherol. J Nutr 2000 Jul;130(7):1649-52.
- Rahman K, et al. Dietary Supplementation with Aged Garlic Extract Inhibits ADP-Induced Platelet Aggregation in Humans. J Nutr 2000 Nov;130(11):2662-2665.
- Kang WS, et al. Antithrombotic activities of green tea catechins and (-)-epigallocatechin gallate. Thromb Res 1999 Nov 1;96(3):229-37.
- Logani S, et al. Actions of Ginkgo Biloba related to potential utility for the treatment of conditions involving cerebral hypoxia. Life Sci 2000 Aug 11;67(12):1389-96.
- Clostre F. [Ginkgo biloba extract (EGb 761). State of knowledge in the dawn of the year 2000]. Ann Pharm Fr 1999 Jul;57 Suppl 1:1S8-88.
- Akisu M, et al. Platelet-activating factor is an important mediator in hypoxic ischemic brain injury in the newborn rat. Flunarizine and Ginkgo biloba extract reduce PAF concentration in the brain. Biol Neonate 1998 Dec;74(6):439-44.
- Lagente V, et al. Effects of the platelet activating factor antagonists BN 52021 and BN 50730 on antigen-induced bronchial hyperresponsiveness and eosinophil infiltration in lung from sensitized guinea-pigs. Clin Exp Allergy 1993 Dec;23(12):1002-10.
- Ceriello A, et al. Total plasma antioxidant capacity predicts thrombosis-prone status in NIDDM patients. Diabetes Care (United States) Oct 1997, 20 (10) p1589-93.
- Vyshevskii ASh, et al. [The role of platelets in the protective effect of a combination of vitamins A, E, C and P in thrombinemia]. Gematol Transfuziol 1995 Sep-Oct;40(5):9-11.
- Ceriello A, et al. Total plasma antioxidant capacity predicts thrombosis-prone status in NIDDM patients. Diabetes Care 1997 Oct;20(10):1589-93.
- Back O, et al. Retinoids and fibrinolysis. Acta Derm Venereol 1995 Jul;75(4):290-2.
- Van Bennekum AM, et al. Modulation of tissue-type plasminogen activator by retinoids in rat plasma and tissues. Am J Physiol 1993 May;264(5 Pt 2):R931-7.
- Thompson EA, et al. Effect of retinoic acid on the synthesis of tissue-type plasminogen activator and plasminogen activator inhibitor-1 in human endothelial cells. Eur J Biochem 1991 Nov 1;201(3):627-32.
- Kooistra T, et al. Stimulation of tissue-type plasminogen activator synthesis by retinoids in cultured human endothelial cells and rat tissues in vivo. Thromb Haemost 1991 May 6;65(5):565-72.
- Oosthuizen W, et al. Both fish oil and olive oil lowered plasma fibrinogen in women with high baseline fibrinogen levels. Thromb Haemost 1994 Oct;72(4):557-62.
- Flaten H, et al. Fish-oil concentrate: effects on variables related to cardiovascular disease. Am J Clin Nutr 1990 Aug;52(2):300-6.
- Midorikawa S, et al. Enhancement by homocysteine of plasminogen activator inhibitor-1 gene expression and secretion from vascular endothelial and smooth muscle cells. Biochem Biophys Res Commun 2000 May 27;272(1):182-5.
- “Teasing out the value of new C-reactive protein test” by Karen Sandrick In CAP Today, 2000 Jan pg 43-47.
- Kaneko K, et al. C-Reactive protein in dilated cardiomyopathy. Cardiology 1999;91(4):215-9.
- Lindahl B, et al. Markers of myocardial damage and inflammation in relation to long-term mortality in unstable coronary artery disease. FRISC Study Group. Fragmin during Instability in Coronary Artery Disease. N Engl J Med 2000 Oct 19;343(16):1139-47.
Wellness
Specialists
1-800-226-2370 - This service is FREE
7:30 AM - 12 AM (ET) Mon-Fri | 9 AM - 12 AM (ET) Sat-Sun