Life Extension Magazine®

WARNING! Normal Blood Pressure May Be High Blood Pressure!
Conventional notions of hypertension overlook the fact that adverse complications of high blood pressure appear at levels far below what most doctors consider “normal.” Here we present the facts and myths about high blood pressure, along with diet and supplement strategies that can help you lower your blood pressure to the safest ranges.
Scientifically reviewed by Dr. Gary Gonzalez, MD, in October 2024. Written by: Dr. William Davis, MD.
Recent advances in medical science make previous notions of hypertension barely recognizable today. Although hypertension is widely misunderstood, often ignored, and generally under-treated, this incredibly important facet of health and well-being can be your passport to cardiovascular disease prevention. High blood pressure can be imperceptible, insidious, and sometimes inscrutable. Too often, people deny that they have high blood pressure. “I’m nervous,” or “I fought traffic to get here,” or “Wait until I relax a little while and it’ll come down,” are common reactions of those advised that their blood pressure is too high. If you truly have high blood pressure, you are not alone. Without intervention, high blood pressure is likely to affect most of us at some point in our lives. With age and declining health, high blood pressure can be as inevitable as death and taxes. Even if you are non-hypertensive at the age of 55, the Framingham Heart Study predicts a 90% likelihood that you’ll be hypertensive within your lifetime. What you need to knowResearch shows that blood pressure related diseases such as a stroke or a heart attack are optimally prevented with blood pressure levels at 115/75. Doctors have allowed a myriad of patients with blood pressure much higher than this to go untreated for years. Alternative methods have been documented to assist in maintaining normal blood pressure.
Too often, discussion about hypertension degenerates into a mandate for prescription medication, once the obligatory comments about eating a healthier diet, reducing salt intake, and quitting smoking are out of the way. It is no secret to the medical community that conventional blood pressure treatment does not fully eliminate the risk of suffering cardiovascular events from hypertension.1 In other words, threats to health from high blood pressure often remain uncorrected even when blood pressure appears to be fully controlled by medication. From Bloodletting to Metabolic SyndromeIn the late nineteenth century, Dr. Carl Ludwig first devised a technique for measuring blood pressure that required the insertion of a tube into an artery, allowing blood to flow into a manometer. Not until the turn of the twentieth century did the sphygmomanometer became available. This device for measuring blood pressure did not require puncturing a blood vessel and was therefore useful for everyday purposes. In 1912, the Massachusetts General Hospital in Boston began mandatory blood pressure measurements for all patients admitted to its wards. Progress in treating high blood pressure has lagged behind techniques for measuring it. Even in Ludwig’s day, some practitioners advocated bloodletting to allow high pressure to dissipate. As recently as the 1960s and 1970s, hospital wards were filled with patients suffering uncontrolled, perilous levels of hypertension (“hypertensive crises”) due to the broad failure of the medical community to recognize and treat earlier phases of high blood pressure. Treatment choices were likewise limited and flawed. Our understanding of blood pressure has advanced considerably since these early observations. Today, medicine has improved, though it is certainly not foolproof. Even better, breakthroughs in the science of regulating blood pressure are revealing many promising nutrition-based approaches for preventing and controlling high blood pressure. Some of the most exciting recent insights revolve around the role of nitric oxide, a master controller of blood pressure, and the frightfully common cluster of health disorders known as metabolic syndrome, an eminently correctable factor in blood pressure control. What Is Normal Blood Pressure?In the 1960s and 1970s, the medical profession used arbitrary guidelines that grossly underestimated the perils of hypertension. For example, a rule practiced in the 1970s held that an “allowable” blood pressure value could be calculated by adding 100 to a person’s age. By this formula, a 60-year-old adult woman would be permitted a systolic blood pressure of 160 mmHg before her physician would become concerned. We all know now that a blood pressure like this virtually guarantees complications of high blood pressure—such as stroke, dementia, and kidney failure—within a few short years.
Why such confusion about acceptable blood pressure levels? The dilemma arises in part because blood pressure is variable. In the morning, just before arising, your systolic/diastolic blood pressure might be 104/78 mmHg. After eating breakfast and having coffee, it could change to 128/74 mm Hg. While sitting at your desk at work, having more coffee, answering email, and making phone calls, your level could rise to 149/79 mmHg. An annoying comment from a customer could push your blood pressure to 164/68 mmHg. After blowing off steam with a friend, walking 200 feet to another part of the building, looking at the picture of your family on your desk, and reminding yourself that there is more to life than work, your blood pressure might then drop to 130/70 mmHg. No one’s blood pressure stays constant at the optimal level of 120/80 mmHg or lower. Blood pressure fluctuates widely, even in people with normal levels. People without high blood pressure will fluctuate into clearly abnormal ranges during periods of emotional stress, overindulgence in unhealthy foods or alcohol, and physically demanding activities. This does not mean they have high blood pressure. Then how do we define high blood pressure if even those with normal blood pressure occasionally trespass into high levels? High blood pressure does not necessarily mean constantly and persistently high. People with high blood pressure tend to fluctuate more widely. Differences of 60-80 mmHg within just a few minutes are common. The “give me a few minutes to calm down” comment that allows systolic blood pressure to drop from 180 to 120 mmHg simply reflects this phenomenon in a hypertensive individual. High blood pressure also stays higher longer and rises above normal more frequently. In other words, for hypertensive people, the peaks and valleys of blood pressure are higher, broader, and more numerous than for those with normal pressure. The ideal way to measure blood pressure is to have somebody follow you throughout the day and measure your blood pressure under all sorts of different circumstances. Unfortunately, this approach is impractical. One practical way to gauge overall blood pressure behavior is to wear an ambulatory blood pressure monitor. This device is worn for 24 hours, and automatically measures and records blood pressure every 15 minutes. Its readings are then reviewed by a physician. Another way is a stress test, since graded exercise’s effects on blood pressure can be observed while the patient walks on a treadmill. Both tests show the extremes of blood pressure fluctuations and offer a good idea of whether you truly have high blood pressure when faced with the stressors of everyday life.
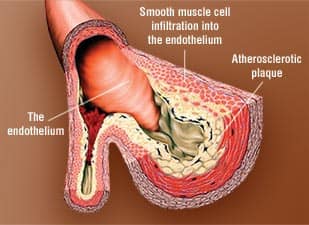
The last option is to simply measure your blood pressure the old-fashioned way, while sitting in your doctor’s office. You can improve on this by adding measures of your own (with an automatic blood pressure cuff or measured by a friend) at different times and under varied circumstances, such as at home, upon awakening, and following exercise. This will gives you a reasonable idea of everyday fluctuations in your blood pressure. However, you should expect variations in pressure, regardless of whether you have high blood pressure. Another reason for confusion over elevated blood pressure arises from its “silent” nature. Only occasionally does high blood pressure cause symptoms like headache or fatigue. The vast majority of those with lurking hypertension feel just fine, with no symptoms at all. Perhaps that is why we question, argue with, and resist a diagnosis of high blood pressure. Blood Pressure’s Ebb and FlowWhat exactly is blood pressure? Put simply, it is the force with which blood is propelled through your arteries. Unlike a river, which flows continuously downstream, blood flow is pulsatile, with the ebb and flow driven by the pumping heart muscle. The heart muscle squeezes forcefully, propelling blood forward. The heart then relaxes and blood flow ebbs momentarily. This cycle repeats itself with each heart-beat, 60 or so times each minute. Blood pressure, therefore, is the pressure contained within your arteries, with a forward burst of flow from heart contraction called systolic pressure, and the receding flow of heart relaxation called diastolic pressure. A blood pressure measurement of 120/80 mmHg signifies a systolic value of 120 and a diastolic value of 80, measured in the pressure units of millimeters of mercury. You can deduce many of the causes of high blood pressure just by understanding this basic process. For instance, pour a greater volume of fluid into the system, and systolic pressure goes up because each contraction of the heart delivers greater volume, and the diastolic pressure goes up because there is more volume to fill the arteries and less room to dissipate pressure during heart relaxation. Several disorders cause fluid retention in your circulatory system and thereby cause high blood pressure. These include excessive salt intake, poor kidney function, and high levels of certain hormones like renin, angiotensin, and cortisol. Another factor is arterial flexibility or stiffness. Normally, arteries are flexible and “give” with pulsatile blood flow. However, when these vessels are stiff, they are less able to expand with bursts of flow, and pressure increases. This is common in arteries lined with semi-rigid atherosclerotic plaque, also known as “hardening” of the arteries. Regardless of their cause, all forms of blood pressure can eventually lead to the same undesirable effects. High blood pressure pounds your organs with each heartbeat, hour after hour, day after day. Over the years, the effects of this relentless trauma begin to show. In the kidney, the ability to filter the body’s waste products and separate excess fluid from blood weakens. In the heart, coronary arteries develop plaque that leads to heart attack. Heart muscle becomes overly thick and muscular, internal heart pressure increases, and you become breathless and retain fluid, a condition called diastolic dysfunction. The arteries of the chest and abdomen, and particularly the major artery of the body, the aorta, also develop plaque. The aorta enlarges, essentially “inflating” under the increased internal pressure of hypertension, leading to the formation of aneurysms. In the brain, the relentless pounding of high blood pressure can lead to deterioration of brain tissue, eventually leading to a form of dementia called multi-infarct dementia that arises from many mini-strokes.
Is “Normal” Blood Pressure Too High?“We have taken it as the natural human condition that blood pressures are as high as they are. We have arbitrarily defined ‘normal blood pressure.’ But that does not mean that normal is optimal.” —Dr. Henry R. Black, Rush University Medical Center At what point does blood pressure begin to have demonstrable effects on cardiovascular complications and mortality itself? At a systolic pressure of 150 mmHg? How about at 140 mmHg? In fact, measurable complications of blood pressure begin to appear at just 115 mmHg! That is, systolic pressures above 115 mmHg are sufficient to generate damage to arteries and other organs, with measurable impacts on morbidity and mortality over a period of several years.2 Every additional increment in blood pressure of 20/10 mmHg doubles one’s risk of developing cardiovascular disease. For this reason, the most recent national guidelines for blood pressure issued by the National Heart, Lung, and Blood Institute recommend maintaining a systolic blood pressure under 120 mmHg and a diastolic pressure below 80 mmHg. Values at or above 140/90 mmHg are considered hypertensive, requiring medical intervention. The new guidelines provide for a category called “pre-hypertension”— defined as systolic pressures of 120-139 mmHg and diastolic pressures of 80-89 mmHg—that justifies lifestyle modification for improvement.1 The recent release of the Camelot Study conducted by Dr. Steven Nissen of the Cleveland Clinic has fueled the argument that lowering blood pressure even moderately yields substantial health benefits. In this study of nearly 2,000 participants with heart disease, lowering blood pressures within the borderline range from 129/78 to 124/76 mmHg led to significant reductions in heart attack, death, and hospitalization. This blood pressure reduction also decreased arterial plaque growth, as measured by intra-coronary ultrasound.3 It is interesting to contemplate what the potential effects of lowering blood pressures to 100 mmHg would be, and perhaps future clinical trials will answer this question for us. Hypertension: A Twenty-First Century EpidemicLook down the aisles at your neighborhood grocery store and you will see why 47 million adults in the US, or about one of every four, have the cluster of disorders dubbed metabolic syndrome. Ninety percent of the products on the supermarket shelves are highly processed foods that are rich in unhealthy fats, loaded with sugar, and depleted of fiber. Combine these foods with lifestyles marked by inactivity, sleep deprivation, and stress, and you create a constellation of physiological phenomena that includes abdominal obesity, low levels of beneficial HDL (high-density lipoprotein), high levels of harmful triglycerides, elevated blood sugar, and high blood pressure. So many adults in the US meet the diagnostic criteria for metabolic syndrome that the total number now afflicted nearly equals the number of “baby boomers.”4 If you have hypertension, there is a high likelihood that you have at least some of the characteristics of metabolic syndrome, particularly resistance to insulin, a condition that precedes development of full-blown diabetes. In fact, the association is so strong that hypertension should be regarded as a significant risk factor for future diabetes, with a greatly increased risk of diabetes in your future.5 Moreover, the estimate of 47 million US adults with metabolic syndrome is based on the rather lax definition of hypertension as a blood pressure greater than 140/90 mmHg. Many truly hypertensive people will be uncounted using this guideline. As noted earlier, blood pressure is, by its nature, labile and variable. It is also clear that blood pressure begins to affect mortality rates at levels above 115 mmHg. Most people are shocked when they hear this, having been accustomed to hypertension guidelines specifying levels of 150/90 mmHg and higher. To remind ourselves of what optimal blood pressure should be, we need only look at blood pressure levels in primitive cultures that lack access to processed foods and are engaged in physical activity much of the day. People in these cultures, who rarely suffer from cardiovascular disease, have blood pressures of around 90/60 mm Hg.2 |
|||||




To Solve Hypertension, Address Metabolic SyndromeMetabolic syndrome is by far the leading trigger for hypertension today. It is also a very correctable cause. Correcting metabolic syndrome can have a tremendous impact on blood pressure. The most powerful way to regain control of multifaceted metabolic syndrome is to lose weight, and there are many ways to do it. People with metabolic syndrome respond especially well to diets that restrict carbohydrates and focus on low “glycemic index” foods that blunt the release of blood sugar. Several low-carb diets are very popular now, largely due to the exaggerated success of carbohydrate restriction in a world overrun with metabolic syndrome.6 These diets come in a variety of names and packages, including Atkins, South Beach, Zone, and others. If you succeed in losing weight on any of these programs, you are very likely to reduce your blood pressure enough (frequently by 10-40 mmHg systolic) to cut down your list of medications. Of course, discontinuing medications should be done only under a doctor’s supervision. If you are contemplating one of these diets but would like to accelerate your weight-loss and metabolic-control efforts, the following supplements and strategies can boost your chances of success. Glucomannan is a unique fiber from konjac root that soaks up huge quantities of water. When taken as a capsule, it provides the effect of filling the stomach and creating a feeling of fullness and satiety. The result is that your appetite is diminished and you eat less. Glucomannan works best when taken before meals with plenty of water. People using glucomannan alone and without a specific diet program generally lose 4-7 pounds a month.7,8 Glucomannan is available in a novel fiber supplement called PGX™. White bean extract can accelerate weight loss, particularly if you have a pattern of low HDL and high triglycerides. A dose of 1500 mg taken twice daily with meals can lead to 3–4 pounds of weight loss in the first month. White bean extract inhibits an enzyme involved in carbohydrate digestion. While some people may experience gas or mild bloating, white bean extract generally has few side effects.9 DHEA’s effects on weight loss have been inconclusive, with some studies demonstrating benefit and others failing to show any difference. However, a recently reported, well-conducted study at Washington University in St. Louis described dramatic results in a group of 56 participants aged 65–78. Over a six-month period, a daily dose of 50 mg of DHEA taken at bedtime yielded significant reductions in abdominal fat (the kind that causes metabolic syndrome) as measured by highly accurate abdominal MRI (magnetic resonance imaging). Along with a loss of abdominal fat, the study’s subjects also saw marked improvement in insulin sensitivity. By contrast, the comparison placebo group experienced an increase in abdominal fat and a deterioration in insulin sensitivity over the same period.10 Although more data are needed, this study argues powerfully in favor of DHEA supplementation to accelerate weight loss, trim abdominal fat, and improve insulin sensitivity. By assisting in weight loss and addressing the symptoms of metabolic syndrome, DHEA holds great promise for helping to manage hypertension. Calcium pyruvate accelerates weight loss, usually cutting a few extra pounds over several weeks, while also making exercise easier and more enjoyable, thus enabling you to exercise longer and harder with faster recovery. Despite its effects in accelerating weight loss, calcium pyruvate is not a stimulant and has been found to be safe and effective.11 Losing weight and improving metabolic syndrome will yield many benefits, including higher HDL, lower triglycerides, less inflammation, improved insulin sensitivity, and lower blood pressure. The amount of weight loss required to improve metabolic syndrome and decrease blood pressure varies among individuals. Some people experience dramatic improvement in all measures with a modest loss of 10 pounds, while others may need to lose significantly more weight to achieve the desired effects. The best course is to work with your physician to devise an effective weight-loss plan.
How Nitric Oxide Controls Blood PressureHigh blood pressure signifies an abnormal tendency for the body’s arteries to constrict. This is true of arteries in the arms and legs, the brain, the heart, and other areas. The ability to correct this abnormal effect may be essential to controlling blood pressure. This insight dates back to 1980, when Dr. Robert Furchgott of the State University of New York conducted experiments on rabbit arteries, trying to decipher how arteries control their state of constriction or tone. Entirely by accident, he noticed that arteries constricted when their inner linings were removed. Dr. Furchgott theorized that the inner lining, or endothelium, is necessary to permit the normal dilating behavior of arteries, and that a damaged endothelium prevents this phenomenon. What followed was a concerted effort to identify the factor or factors produced by the endothelium that governed relaxation. Dr. Furchgott originally called this mysterious substance “endothelium-derived relaxation factor,” or EDRF. For several years, identification of EDRF proved elusive, as it persisted for a mere few seconds before disappearing.12 In 1986, EDRF was discovered to be nitric oxide.13 This discovery initially drew skepticism, as nitric oxide is a common gaseous byproduct of nitrogen combustion, which is plentiful in automobile exhaust. How could it be the critical cellular messenger controlling arterial tone? Dr. Furchgott’s discovery has endured intense scrutiny and was honored by the 1998 Nobel Prize for Medicine, which he shared with his colleagues Drs. Louis Ignarro and Ferid Murad for their related work. Today, nitric oxide is recognized as the signaling molecule for many physiological processes, as well as the single most powerful artery-dilating agent known to medicine.12-14 “We now know that the endothelium exerts tremendous control over blood flow. First, its prime location plays a role. Because the endothelium is the inner-most lining of the blood vessel, it has direct contact with blood and, as such, serves as an interface between the blood and the vessel wall . . . We now know that this delicate tissue, only one cell layer in thickness, is a dynamic factory, producing a myriad of substances that maintain vessel health. It is, in essence, a silver lining—since when it’s healthy, it produces its own forms of heart medicine.” —Dr. John Cooke, Because of nitric oxide’s extremely short life of no more than 10 seconds, a constant supply is required to keep arteries dilated and relaxed. Any drop in nitric oxide production causes arteries to constrict. Cholesterol abnormalities, high blood pressure, inflammation, high blood sugar or diabetes, a high-fat diet, and sugary, refined foods all impair the endothelial cells’ ability to produce nitric oxide. Metabolic syndrome has the same effect, leading to repeated damage to the artery linings that triggers atherosclerotic plaque formation, or “endothelial dysfunction.” When arteries are lined with even a microscopically thin layer of plaque, they are less able to produce nitric oxide, yielding even more injury.
How can factors as diverse as diabetes, fatty foods, and inflammation all disrupt the endothelium’s control over arterial relaxation? Much of this abnormal arterial constriction, or endothelial dysfunction, occurs in situations involving high cholesterol, high blood pressure, high triglycerides, diabetes and insulin resistance, high homocysteine, and atherosclerotic plaque.15-18 What About Antioxidants?In addition to the previously discussed mechanisms, hypertension may also be induced by the presence of oxidative stressors. This theory arises from the observation that hypertension can be produced experimentally by various oxidative molecules, such as superoxide. Superoxide disables the vasodilator nitric oxide by forming peroxynitrite, a potent constrictor of arteries.19 Thus, antioxidants may play a role in maintaining healthy blood pressure levels. Vitamin C is an antioxidant whose role in helping to regulate blood pressure has been the subject of numerous of clinical trials. To date, the study results have been mixed, with some showing that vitamin C reduces blood pressure and others showing no effect.20 Based on existing clinical studies, the one antioxidant that stands out as truly effective by itself in lowering blood pressure is coenzyme Q10 (CoQ10). Eight studies have examined CoQ10’s effects on blood pressure, and the pooled data show that CoQ10 supplementation helped lower systolic pressure by an impressive 16 mmHg and diastolic pressure by 10 mmHg. The doses studied generally ranged from 50 to 200 mg a day.21 Recent reports have suggested that lowering blood pressure is not enough to eliminate high blood pressure’s contribution to cardiovascular events such as heart attack and death. Reduction of abnormal heart muscle thickening, or “hypertrophy,” as measured by ultrasound, may also be a necessary component of treatment.22 This effect is not accomplished by every prescription antihypertensive medication. Interesting data from the University of Texas-Austin suggest that abnormal hypertrophy resulting from high blood pressure can be substantially regressed with CoQ10 treatment.23,24 ConclusionThe growing prevalence of metabolic syndrome has made it an increasingly important contributor to hypertension. Metabolic syndrome is a controllable and largely correctable condition. Weight loss is the principal means of regaining control over this process, by improving blood pressure and numerous other markers of health. Antioxidant research has great potential in the field of blood pressure control. By reducing such blood vessel constrictors as the oxidant peroxynitrite, antioxidants may hold great benefits for the cardiovascular system. In particular, significant data support the use of coenzyme Q10 for reducing blood pressure. Hypertension is a silent, potentially deadly condition that affects millions of Americans. Through a combination of lifestyle modifications and nutritional strategies, it is possible to improve your blood pressure by natural means. Optimizing blood pressure is a critical part of a daily wellness program for those seeking to live long, healthy lives. Dr. William Davis is an author, lecturer, and practicing cardiologist focusing on coronary disease regression. He is the author of the book Track Your Plaque. He can be contacted at www.trackyourplaque.com. Editor's Note: Science continues to evolve, and new research is published daily. As such, we have a more recent article on this topic here: Around-the-Clock Blood-Pressure Control | ||||
| References | ||||
|

Wellness
Specialists
1-800-226-2370 - This service is FREE
7:30 AM - 12 AM (ET) Mon-Fri | 9 AM - 12 AM (ET) Sat-Sun