Life Extension Magazine®
One of the most frequent causes of hospital admissions in older adults is the devastating condition known as congestive heart failure. Characterized by disabling symptoms of difficulty breathing, fatigue, and swelling of the extremities, congestive heart failure also increases the risk of early demise. Fortunately, scientists have discovered that the mitochondrial energizer coenzyme Q10 (CoQ10) can offer powerful assistance to those challenged with congestive heart failure, improving the heart’s pumping ability and even reducing the need for medications. Since CoQ10 levels are depleted by aging and statin medications and tend to be low in those with congestive heart failure, achieving optimal blood levels of CoQ10 may be an important strategy for safeguarding cardiac health. What is CoQ10?It has been 50 years since Fred Crane discovered CoQ10 in 1957.1 Since that time, scientists have discovered what this extraordinary molecule is and what it does in settings of both health and disease. It is important to clarify that a coenzyme should not be confused with an enzyme (a protein that accelerates a biochemical reaction). A coenzyme is a simple molecule (many vitamins are coenzymes) that is essential for the normal function of specific enzyme systems in our cells. Coenzyme Q10 is the cofactor or coenzyme for three large enzyme systems that are essential for 90% of cellular energy production. Because the heart muscle uses more energy than any other tissue and normally has the highest concentration of CoQ10, it is very sensitive to CoQ10 deficiency.
Coenzyme Q10 is well established to be a clinically relevant first-line antioxidant in our defense system against excess oxidative stress. It is the only fat-soluble antioxidant that is synthesized by our body and is capable of regeneration back to its reduced or antioxidant form through normal cellular enzyme systems. Its location in the lipid mitochondrial membranes is particularly important, as mitochondria are the major site of free-radical production, and CoQ10 is an excellent free-radical scavenger. Coenzyme Q10 and Congestive Heart FailureIn the late 1960s and early 1970s, it became clear that patients suffering from congestive heart failure had measurable deficiency of CoQ10 in both blood and heart muscle, and that the degree of deficiency correlated with the severity of heart failure. Much of this work was performed as a collaborative effort between Professor Karl Folkers, PhD, Gian Paolo Littarru, MD, and Denton Cooley, MD.2 In 1980, my father, cardio-logist Per H. Langsjoen, MD, met with Karl Folkers, and together they performed the first human trial of CoQ10 in the treatment of congestive heart failure in the United States.3 I joined my father as a cardiology fellow in 1983 and after this favorable controlled study was published in 1985, we went on to evaluate the long-term efficacy of CoQ10 therapy in 126 patients with congestive heart failure.4
Congestive heart failure is a condition in which there is weakening of heart muscle function so that fluid or congestion backs up and causes swelling or edema in the liver, lungs, the lining of the intestine, and the lower legs and feet. It was our initial concern that CoQ10 may have been acting as a stimulant that could bring about short-term improvement in heart muscle function but actually increase mortality over time. This is similar to flogging an exhausted horse, making him run faster for a few hundred yards only to promptly drop dead. By following these 126 heart failure patients for six years, it became clear that the improvement in heart function was sustained and that overall mortality was one third of expected.4 It was at this time that we realized CoQ10 represented a major advance in the treatment of a disease that previously could be only palliated and never cured. In the course of this six-year study, the 126 patients were followed very closely with measurement of blood CoQ10 levels and heart function every three months.4 We unexpectedly came across the detrimental effect of the cholesterol-lowering drugs known as HMG-CoA reductase inhibitors, or more simply as statins. The first statin drug, lovastatin (Mevacor®) came on the market in 1987, and five of our heart failure patients were started on this drug by their primary care physicians. All five of these stabilized patients had a significant decline in their blood CoQ10 levels and a decline in their heart function and clinical status. Their heart failure worsened to such a degree that two patients became critically ill and one went on to require a heart transplant. This clinical deterioration in our patients was particularly frightening at the time because we had no idea of the dramatic CoQ10-depleting effects of the newly released statin drugs. One patient in particular showed a simultaneous drop in plasma CoQ10 level and ejection fraction when started on statin therapy, with improvement after the statin was discontinued (see figure 1). My father first presented these data in Rome, Italy, in January of 1990.5 Shortly after my father left the podium, a member of the audience shouted into one of the aisle microphones, “This is pharmaceutical terrorism!” To which my father calmly responded, “Yes, but who is the terrorist?” Later that year in May and in June of 1990, Merck went on to secure two patents that would combine CoQ10 with statin drugs in the same capsule to prevent muscle and liver damage.6 The first of these patents was with co-inventor Michael Brown of Nobel Laureate fame for his work with low-density lipoprotein (LDL) receptors. Unfortunately, these patents have never been acted on and to this day, the vast majority of physicians and patients are completely unaware of statin-induced CoQ10 depletion. The Trouble with StatinsAll statin drugs block the biosynthesis of both cholesterol and CoQ10, which explains statins’ common side effects of fatigue, muscle pain and muscle weakness, and a worsening of heart failure (see figure 2).
When CoQ10 levels are lowered by statin drug therapy, one of the first changes to occur is a weakening of heart muscle function, known as diastolic dysfunction. This has nothing to do with diastolic blood pressure, but rather represents impairment in the relaxing or filling phase of the cardiac cycle. After heart muscle contracts, it takes a great deal of cellular energy, or ATP, to re-establish the calcium gradients such that muscle fibers may relax. Thus, if diastolic dysfunction is severe, it can result in congestive heart failure. In 2004, a study published in the American Journal of Cardiology showed that diastolic dysfunction (heart muscle weakness) occurred in 70% of previously normal patients treated with 20 mg a day of Lipitor® for six months. This heart muscle dysfunction was reversible with supplemental CoQ10.7 Heart failure that develops after years of statin drug therapy can be termed statin cardiomyopathy and may well be playing a role in the epidemic of congestive heart failure in the United States. It is important for the reader to be aware that for every adverse side effect caused by statin drug therapy, one can find a drug company-sponsored trial concluding that statins actually benefit the condition they may induce. Good examples are studies that suggest statins are useful in the treatment of cancer,8 when in fact some studies suggest that they could be carcinogenic;9,10 another study suggests that statin therapy may be helpful in dementia,11 when other evidence indicates that statins impair mental function;12,13 finally, studies that conclude statin therapy improves heart failure,14 when in fact it appears to weaken both skeletal muscle and heart muscle.7,15 In an effort to determine the prevalence of adverse effects from using statins, we studied 50 consecutive new patients, all of whom were taking a statin drug at the time of their initial visit.16 All 50 patients were found to have one or more side effects from statin therapy, so we discontinued their statin drugs and began supplemental CoQ10. Patients were followed for an average of 28 months with the following observations in the prevalence of adverse effects:
There were no adverse effects from stopping statin drug therapy with no cases of heart attack or stroke during follow-up. Overall, there was an improvement in heart muscle function on discontinuation of statin therapy and addition of supplemental CoQ10. However, due to powerful propaganda surrounding both cholesterol and statin drug therapy, many patients and physicians are afraid to stop statin therapy. Cholesterol and Heart DiseaseAtherosclerosis remains a disease of unknown cause. Many factors more important than cholesterol—such as stress, smoking, hypertension, insulin resistance, high triglycerides, diabetes, and low testosterone (in men)—contribute to atherosclerosis and cardiovascular disease.17-19 Despite this, the theory that cholesterol is the dominant villain responsible for atherosclerosis has been promulgated for over 60 years, making the pharmaceutical industry’s anti-cholesterol campaign the most profitable medical myth of all time. Statin drugs do show some benefit in reducing mortality in individuals with pre-existing coronary artery disease.20 This benefit occurs irrespective of cholesterol lowering and is likely secondary to their subtle anti-inflammatory or plaque-stabilizing effects.21 The vilification of cholesterol and the associated aggressive lowering of cholesterol blood levels has brought about increasingly severe CoQ10 deficiency in a large number of patients, making it absolutely critical to restore CoQ10 levels in these individuals. Optimal CoQ10 Levels Improve Heart FailureIn the early years of our experience with CoQ10 therapy, no one knew the therapeutic or ideal plasma level of CoQ10 for the treatment of heart failure. Over the course of 25 years, it has become clear that maximum improvement in heart function will not occur unless plasma levels are greater than 3.5 micrograms per milliliter (mcg/mL). By 2006, there were a total of 22 randomized, controlled trials involving a total of 1,605 patients evaluating the therapeutic benefit of supplemental CoQ10 in congestive heart failure.22-24 The majority of studies were favorable, showing significant improvement in heart muscle function. Furthermore, there have been 34 open-label trials involving 4,221 patients evaluating the clinical utility of CoQ10 in heart failure, and again clear benefits were observed without any adverse effect or drug interaction. Despite these studies, CoQ10 remains obscure to most physicians and is not routinely used in the treatment of congestive heart failure. This is in part due to the pervasive anti-nutrient bias in conventional medical practice, medical literature, and medical education. Out of a total of 22 controlled trials of supplemental CoQ10 in congestive heart failure, only three have failed to show significant benefit. The first study by Permanetter et al. failed to measure plasma CoQ10 levels, such that there is no way to know if therapeutic CoQ10 levels were attained.25 The second trial by Watson et al. demonstrated a mean treatment plasma CoQ10 level of only 1.7 mcg/mL, with only two of the 30 patients having a plasma level greater than 2.0 mcg/mL.26 Finally, the third study by Khatta et al. demonstrated a mean treatment plasma CoQ10 level of 2.2 ± 1.2 mcg/mL, indicating that some patients on treatment had levels as low as 1.0 mcg/mL.27 Unfortunately, these last two trials with sub-therapeutic CoQ10 levels are the most frequently quoted as evidence for a lack of benefit for CoQ10 in heart failure | ||||||||



Absorption of CoQ10
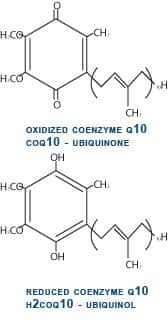
From the beginning of our experience with CoQ10 in heart failure, we have observed poor absorption of CoQ10 in patients with advanced congestive heart failure. This is extremely frustrating, because the patients who are the most ill and have the lowest plasma CoQ10 levels show minimal improvement because of their inability to absorb CoQ10. It has been our assumption that the fluid retention or edema in the intestine and liver in these critically ill patients has been responsible for this poor absorption. Up until approximately one year ago, all supplemental CoQ10 in the world has been in its oxidized or ubiquinone form. In this oxidized state, CoQ10 is stable, bright orange in color, and fat-soluble. It is this property of being fat-soluble that is responsible for the difficulty with CoQ10 absorption. A Better Form of CoQ10After ingestion, immediately after CoQ10 crosses into the first cells lining the small intestine, it is enzymatically converted to its reduced, or ubiquinol, form. So, when we measure plasma CoQ10, approximately 98-99% of the CoQ10 is in this reduced ubiquinol form (see figure 3). Kaneka Corporation of Japan has succeeded in making a stable ubiquinol formulation that we have been carefully studying since October 2006. Ubiquinol is a white powder rather than orange and is less fat-soluble, making it better absorbed. Our first patient to be treated with ubiquinol had severe heart failure with a 15% ejection fraction (a measurement of the amount of blood pumped out with each heartbeat, which is normally 60-65%). This gentleman had a sub-therapeutic plasma CoQ10 level of 2.2 mcg/mL on 450 mg per day of ubiquinone. His plasma level on 450 mg per day of ubiquinol increased dramatically to 8.5 mcg/mL and over the subsequent 10 months, his ejection fraction increased to 60% with a corresponding dramatic and perhaps life-saving clinical improvement (see figure 4). We now have a total of seven patients with advanced congestive heart failure and low plasma CoQ10 levels, despite taking as much as 600 mg per day of ubiquinone (the oxidized form of CoQ10) who have been changed over to the ubiquinol (the reduced form) formulation. Our preliminary observations have been very favorable, and it is my strong opinion that supplemental ubiquinol represents a major scientific advance in the 50-year history of CoQ10 research. Supplementing with CoQ10
I would like to make a few practical comments based on 24 years of treating thousands of heart failure patients with supplemental CoQ10 in addition to standard prescription medications. We have seen no side effects and no drug interactions from supplemental CoQ10, but we have observed a gradual lessening of the requirement for many cardiac medications that occurs with an improvement in heart muscle function. For example, we have observed a significant decrease in the need for diuretics, because of a reduced tendency for fluid retention as heart function improves. Also, we have noted a gradual improvement in hypertension that occurs as heart function improves, which may require a gradual decrease in antihypertensive medications such as angiotensin-converting enzyme (ACE) inhibitors, a class of blood pressure-lowering medicines frequently used in heart failure patients. Patients with heart disease should be followed by their physicians, particularly when there are any changes in activity, diet, prescription drugs, or over-the-counter supplements. I have treated hundreds of patients with CoQ10 and have never observed an interaction with warfarin (Coumadin®). There have been anecdotal reports that the combination may increase the risk of bleeding. Individuals who use warfarin should always consult a physician before using CoQ10.28,29 Choosing a CoQ10 Formulation and DosageMost commercially available CoQ10 supplements comprise ubiquinone. Recommended daily dosages of this type of CoQ10 range from 100 mg to 600 mg. The most advanced CoQ10 formulas now contain ubiquinol, the reduced form of CoQ10, which is definitely better absorbed into the bloodstream.30-32 Recommended daily dosages of ubiquinol range from 100 mg to 300 mg. Because we know that CoQ10 levels tend to decrease with age and we live in a society that consumes very little food rich in CoQ10 (organ meats like heart, liver, and kidney), it makes sense to supplement with a modest amount of CoQ10 (ubiquinone or ubiquinol) beginning in middle age. Those who suffer from congestive heart failure or who use statin medications should aim to consume higher doses of CoQ10 (ubiquinone or ubiquinol). ConclusionCoenzyme Q10’s ability to fundamentally improve the production of energy and the antioxidant defense in every cell of the body has brought about many remarkable and unexpected improvements in all aspects of human health. This extraordinary molecule has dramatically changed my own practice of medicine and has brought joy to the treatment of previously devastating cardiovascular diseases. If you have any questions on the scientific content of this article, please call a Life Extension Health Advisor at 1-800-226-2370. | ||||||||
| References | ||||||||
| 1. Crane FL, Hatefi Y, Lester RL, Widmer C. Isolation of a quinone from beef heart mitochondria. Biochim Biophys Acta. 1957 Jul;25(1):220-1. 2. Folkers K, Littarru GP, Ho L, et al. Evidence for a deficiency of coenzyme Q10 in human heart disease. Int Z Vitaminforsch. 1970;40(3):380-90. 3. Langsjoen PH, Vadhanavikit S, Folkers K. Response of patients in classes III and IV of cardiomyopathy to therapy in a blind and crossover trial with coenzyme Q10. Proc Natl Acad Sci USA. 1985 Jun;82(12):4240-4. 4. Langsjoen PH, Langsjoen PH, Folkers K. Long-term efficacy and safety of coenzyme Q10 therapy for idiopathic dilated cardiomyopathy. Am J Cardiol. 1990 Feb 15;65(7):521-3. 5. Folkers K, Langsjoen P, Willis R, et al. Lovastatin decreases coenzyme Q levels in humans. Proc Natl Acad Sci USA. 1990 Nov;87(22):8931-4. 6. US Patent 4929437, issued May 29, 1990 and US Patent 4933165, issued June 12, 1990, both titled “Coenzyme Q10 with HMG-CoA Reductase Inhibitors.” 7. Silver MA, Langsjoen PH, Szabo S, Patil H, Zelinger A. Effect of atorvastatin on left ventricular diastolic function and ability of coenzyme Q10 to reverse that dysfunction. Am J Cardiol. 2004 Nov 15;94(10):1306-10. 8. Hindler K, Cleeland CS, Rivera E, Collard CD. The role of statins in cancer therapy. Oncologist. 2006 Mar;11(3):306-15. 9. Alsheikh-Ali AA, Maddukuri PV, Han H, Karas RH. Effect of the magnitude of lipid lowering on risk of elevated liver enzymes, rhabdomyolysis, and cancer: insights from large randomized statin trials. J Am Coll Cardiol. 2007 Jul 31;50(5):409-18. 10. Newman TB, Hulley SB. Carcinogenicity of lipid-lowering drugs. JAMA. 1996 Jan 3;275(1):55-60. 11. Li G, Larson EB, Sonnen JA, et al. Statin therapy is associated with reduced neuropathologic changes of Alzheimer disease. Neurology. 2007 Aug 28;69(9):878-85. 12. Golomb BA, Jaworski B. Statins and dementia. Arch Neurol. 2001 Jul;58(7):1169-70. 13. Padala KP, Padala PR, Potter JF. Simvastatin-induced decline in cognition. Ann Pharmacother. 2006 Oct;40(10):1880-3. 14. Kurian KC, Rai P, Sankaran S, et al. The effect of statins in heart failure: beyond its cholesterol-lowering effect. J Card Fail. 2006 Aug;12(6):473-8. 15. Phillips PS, Haas RH, Bannykh S, et al. Statin-associated myopathy with normal creatine kinase levels. Ann Intern Med. 2002 Oct 1;137(7):581-5. 16. Langsjoen PH, Langsjoen JO, Langsjoen AM, Lucas LA. Treatment of statin adverse effects with supplemental Coenzyme Q10 and statin drug discontinuation. Biofactors. 2005;25(1-4):147-52. 17. Bartnik M, Norhammar A, Rydén L. Hyperglycaemia and cardiovascular disease. J Intern Med. 2007 Aug;262(2):145-56. 18. Le NA, Walter MF. The role of hypertriglyceridemia in atherosclerosis. Curr Atheroscler Rep. 2007 Aug;9(2):110-5. 19. Available at: http://circ.ahajournals.org/cgi/content/abstract.Accessed November 29, 2007. 20. Allen Maycock CA, Muhlestein JB, Horne BD, et al. Statin therapy is associated with reduced mortality across all age groups of individuals with significant coronary disease, including very elderly patients. J Am Coll Cardiol. 2002 Nov 20;40(10):1777-85. 21. Sorrentino S, Landmesser U. Nonlipid-lowering effects of statins. Curr Treat Options Cardiovasc Med. 2005 Dec;7(6):459-66. 22. Langsjoen PH, Langsjoen AM. Overview of the use of CoQ10 in cardiovascular disease. Biofactors. 1999;9(2-4):273-84. 23. Langsjoen PH, Littarru GP, Silver MA. Role of concomitant coenzyme Q10 with statins for patients with hyperlipidemia. Curr Topics Nutr Res. 2005;3(3):149-58. 24. Langsjoen PH, Langsjoen AM. Coenzyme Q10 in cardiovascular disease with emphasis on heart failure and myocardial ischaemia. Asia Pacific Heart J. 1998;7(3):160-8. 25. Permanetter B, Rössy W, Klein G, Weingartner F, Seidl KF, Blömer H. Ubiquinone (coenzyme Q10) in the long-term treatment of idiopathic dilated cardiomyopathy. Eur Heart J. 1992 Nov;13(11):1528-33. 26. Watson PS, Scalia GM, Gaibraith AJ, Burstow DJ, Aroney CN, Bett JH. Is coenzyme Q10 helpful for patients with idiopathic cardiomyopathy? Med J Aust. 2001 Oct 15;175(8):447; author reply 447-8. 27. Khatta M, Alexander BS, Krichten CM, et al. The effect of coenzyme Q10 in patients with congestive heart failure. Ann Intern Med. 2000 Apr 18;132(8):636-40. 28. Shalansky S, Lynd L, Richardson K, Ingaszewski A, Kerr C. Risk of warfarin-related bleeding events and supratherapeutic international normalized ratios associated with complementary and alternative medicine: a longitudinal analysis. Pharmacotherapy. 2007 Sep;27(9):1237-47. 29. Engelsen J, Nielsen JD, Winther K. Effect of coenzyme Q10 and ginkgo biloba on warfarin dosage in stable, long-term warfarin treated outpatients. A randomised, double blind, placebo-crossover trial. Thromb Haemost. 2002 Jun;87(6):1075-6. 30. Hosoe K, Kitano M, Kishida H, Kubo H, Fujii K, Kitahara M. Study on safety and bioavailability of ubiquinol (Kaneka QH (trade mark)) after single and 4-week multiple oral administration to healthy volunteers. Regul Toxicol Pharmacol. 2007 Feb;47(1):19-28. 31. Shults CW, Oakes D, Kieburtz K, et al. Effects of coenzyme Q10 in early Parkinson disease: evidence of slowing of the functional decline. Arch Neurol. 2002 Oct;59(10):1541-50. 32. Shults CW, Flint BM, Song D, Fontaine D. Pilot trial of high dosages of coenzyme Q10 in patients with Parkinson’s disease. Exp Neurol. 2004 Aug;188(2):491-4. |

Wellness
Specialists
1-800-226-2370 - This service is FREE
7:30 AM - 12 AM (ET) Mon-Fri | 9 AM - 12 AM (ET) Sat-Sun